

2D kV orthogonal imaging with fiducial markers is more precise for daily image guided alignments than soft-tissue cone beam computed tomography for prostate radiation therapy
- PMID: 29114611
- PMCID: PMC5605315
- DOI: 10.1016/j.adro.2017.05.001
2D kV orthogonal imaging with fiducial markers is more precise for daily image guided alignments than soft-tissue cone beam computed tomography for prostate radiation therapy
Abstract
Purpose: The hypothesis is that 2-dimensional kV orthogonal imaging with fiducial markers (kV-FM) and soft-tissue cone beam computed tomography (ST-CBCT) are equally reproducible for daily positional alignments for image guided (IG) intensity modulated radiation therapy (IMRT) for prostate cancer.
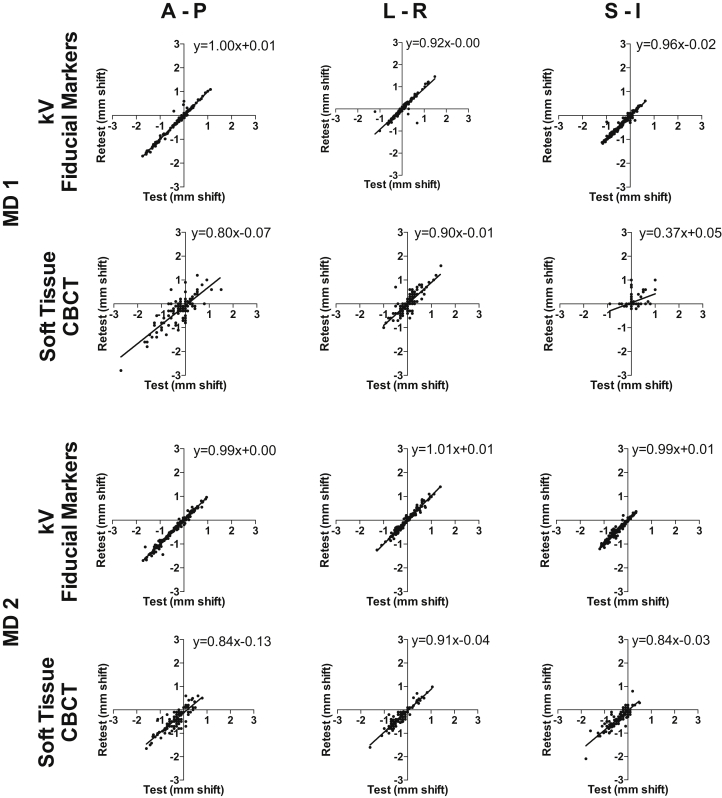
Methods and materials: Ten patients undergoing definitive treatment for prostate cancer with IG-IMRT were imaged daily with kV-FM and ST-CBCT. For each acquired kV and CBCT image, offline alignments to the digitally reconstructed radiograph or planning CT, respectively, were made twice by the same physician to assess intraobserver test-retest reproducibility. The 256 kV and 142 CBCT images were analyzed, and the test-retest analysis was performed again on a subset of images by another physician to verify the results.
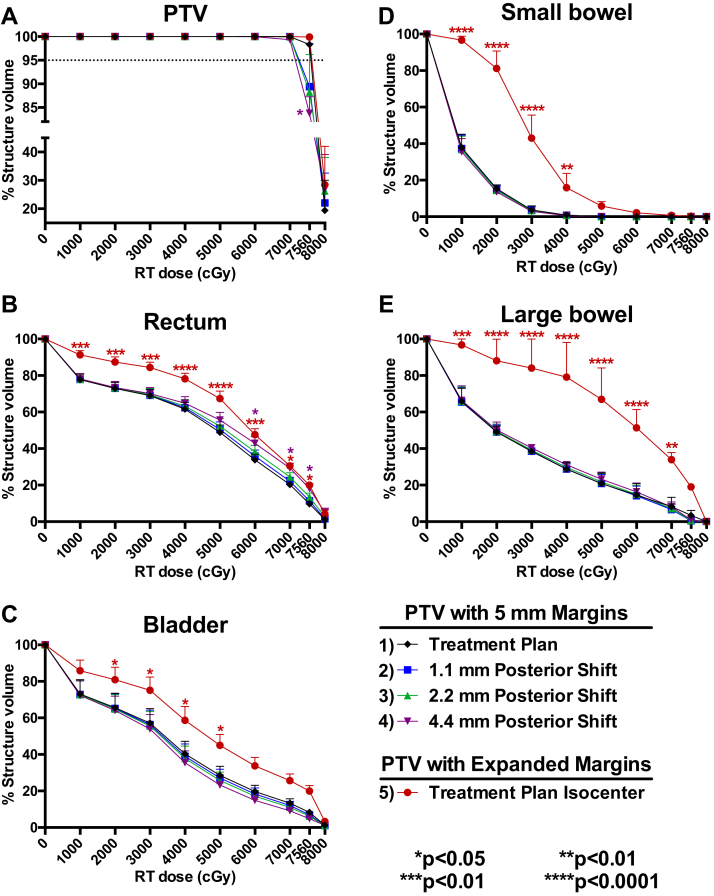
Results: The results demonstrated that kV-FM had better intraobserver test-retest reproducibility in the anterior-posterior (AP; 95% confidence interval [CI] Pearson correlation coefficient [r], 0.987-0.991), left-right (LR; 95% CI r, 0.955-0.969), and superior-inferior (SI; 95% CI r, 0.971-0.980) directions for daily IG alignments compared with ST-CBCT (AP: 95% CI r, 0.804-0.877; LR: 95% CI r, 0.877-0.924; SI: 95% CI r, 0.791-0.869). Errors associated with intraobserver test-retest reproducibility were submillimeter with kV-FM (AP: 0.4 ± 0.7 mm; RL: 0.4 ± 1.0 mm; SI: 0.5 ± 0.7 mm) compared with ST-CBCT (AP: 2.1 ± 2.2 mm; LR: 1.3 ± 1.4 mm; SI: 1.2 ± 1.8 mm). The mean shift differences between kV-FM and ST-CBCT were 0.3 ± 3.8 mm for AP, -1.1 ± 8.5 mm for LR, and -2.0 ± 3.7 mm for SI. Dose-volume histograms were generated and showed that test-retest variability associated with ST-CBCT IG-alignments resulted in significantly increased dose to normal structures and a reduced planning target volume dose in many patients.
Conclusions: The kV-FM-based daily IG alignment for IMRT of prostate cancer is more precise than ST-CBCT, as assessed by a physician's ability to reproducibly align images. Given the magnitude of the error introduced by inconsistency in making ST-CBCT alignments, these data support a role for daily kV imaging of FM to enhance the precision of external beam dose delivery to the prostate.
Figures
Similar articles
-
The potential failure risk of the cone-beam computed tomography-based planning target volume margin definition for prostate image-guided radiotherapy based on a prospective single-institutional hybrid analysis.Radiat Oncol. 2018 Jun 7;13(1):106. doi: 10.1186/s13014-018-1043-9. Radiat Oncol. 2018. PMID: 29880006 Free PMC article.
-
Comparison of kV Orthogonal Radiographs and kV-Cone-Beam Computed Tomography Image-Guided Radiotherapy Methods With and Without Implanted Fiducials in Prostate Cancer.Cureus. 2020 Aug 21;12(8):e9916. doi: 10.7759/cureus.9916. Cureus. 2020. PMID: 32850264 Free PMC article.
-
Image-guided radiotherapy (IGRT) for prostate cancer comparing kV imaging of fiducial markers with cone beam computed tomography (CBCT).Int J Radiat Oncol Biol Phys. 2011 May 1;80(1):301-5. doi: 10.1016/j.ijrobp.2010.06.007. Epub 2010 Sep 23. Int J Radiat Oncol Biol Phys. 2011. PMID: 20864274
-
The impact of the three degrees-of-freedom fiducial marker-based setup compared to soft tissue-based setup in hypofractionated intensity-modulated radiotherapy for prostate cancer.J Appl Clin Med Phys. 2019 Jun;20(6):53-59. doi: 10.1002/acm2.12603. Epub 2019 May 4. J Appl Clin Med Phys. 2019. PMID: 31054217 Free PMC article.
-
Comparison of localization performance with implanted fiducial markers and cone-beam computed tomography for on-line image-guided radiotherapy of the prostate.Int J Radiat Oncol Biol Phys. 2007 Mar 1;67(3):942-53. doi: 10.1016/j.ijrobp.2006.10.039. Int J Radiat Oncol Biol Phys. 2007. PMID: 17293243 Free PMC article.
Cited by
-
Five Fractions versus Seven Fractions SBRT for Intermediate- and High-Risk Prostate Cancer: A Propensity Score Matched Pair Analysis.Cancers (Basel). 2023 Dec 12;15(24):5815. doi: 10.3390/cancers15245815. Cancers (Basel). 2023. PMID: 38136360 Free PMC article.
-
Daily Image Guidance With Cone Beam Computed Tomography May Reduce Radiation Pneumonitis in Unresectable Non-Small Cell Lung Cancer.Int J Radiat Oncol Biol Phys. 2018 Aug 1;101(5):1104-1112. doi: 10.1016/j.ijrobp.2018.03.025. Epub 2018 Mar 30. Int J Radiat Oncol Biol Phys. 2018. PMID: 29730063 Free PMC article.
-
Treatment efficiency and quality improvement via double imaging modality (DIM) versus single imaging modality (SIM) image-guided radiotherapy for prostate cancer.Tech Innov Patient Support Radiat Oncol. 2025 Feb 21;33:100307. doi: 10.1016/j.tipsro.2025.100307. eCollection 2025 Mar. Tech Innov Patient Support Radiat Oncol. 2025. PMID: 40092911 Free PMC article.
-
Dose reduction potential of using gold fiducial markers for kilovoltage image-guided radiotherapy.J Appl Clin Med Phys. 2020 Oct;21(10):151-157. doi: 10.1002/acm2.13023. Epub 2020 Sep 22. J Appl Clin Med Phys. 2020. PMID: 32959957 Free PMC article.
-
Intrafraction Imaging Can Replace the Midtreatment Cone Beam Tomography for Lung Stereotactic Ablative Radiation Therapy Patients for Increased Treatment Efficiency.Adv Radiat Oncol. 2023 Nov 2;9(3):101397. doi: 10.1016/j.adro.2023.101397. eCollection 2024 Mar. Adv Radiat Oncol. 2023. PMID: 38304113 Free PMC article.
References
-
- Howlader N., Noone A.M., Krapcho M. SEER Cancer Statistics Review, 1975-2013, National Cancer Institute. http://seer.cancer.gov/csr/1975_2013/ Available at: Accessed June 21, 2017.
-
- Cahlon O., Zelefsky M.J., Shippy A. Ultra-high dose (86.4 Gy) IMRT for localized prostate cancer: Toxicity and biochemical outcomes. Int J Radiat Oncol Biol Phys. 2008;71:330–337. - PubMed
-
- Zelefsky M.J., Levin E.J., Hunt M. Incidence of late rectal and urinary toxicities after three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys. 2008;70:1124–1129. - PubMed
-
- Michalski J.M., Yan Y., Watkins-Bruner D. Preliminary toxicity analysis of 3-dimensional conformal radiation therapy versus intensity modulated radiation therapy on the high-dose arm of the Radiation Therapy Oncology Group 0126 prostate cancer trial. Int J Radiat Oncol Biol Phys. 2013;87:932–938. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
