

doi: 10.1001/jamainternmed.2017.5960.
Trends in Inferior Vena Cava Filter Placement by Indication in the United States From 2005 to 2014
Affiliations
- PMID: 29114739
- PMCID: PMC5820719
- DOI: 10.1001/jamainternmed.2017.5960
Item in Clipboard
Trends in Inferior Vena Cava Filter Placement by Indication in the United States From 2005 to 2014
JAMA Intern Med.
.
Abstract
This population-based study examines the change in the rates of inferior cava filter placement in US inpatients from 2005 to 2014.
Conflict of interest statement
Figures
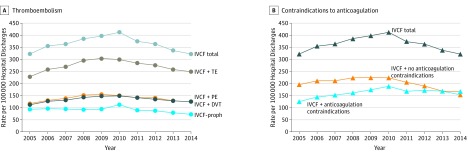
A, Rates with and without thromboembolism (TE) per 100 000 hospital discharges by year. B, Rates with and without contraindications to anticoagulation (eg, intracranial bleeding, other major bleeding, thrombocytopenia, active gastrointestinal tract ulcer, hemophilia, von Willebrand disease, cerebral aneurysm, aortic dissection, pericardial disease, bacterial endocarditis, preeclampsia or eclampsia, malignant hypertension, brain surgery, spinal surgery, or eye surgery) per 100 000 hospital discharges by year. DVT indicates deep vein thrombosis without pulmonary embolism; PE, pulmonary embolism; and proph, prophylactic.
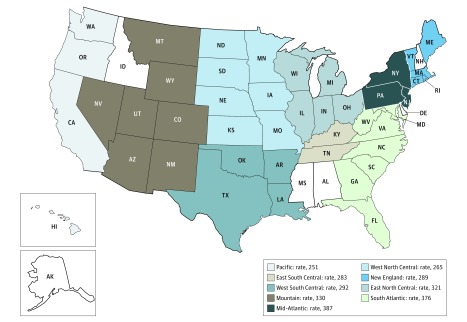
Data from 2014 US Census Division. New England: Connecticut, Maine, Massachusetts, New Hampshire,a Rhode Island, and Vermont. Mid-Atlantic: New Jersey, New York, and Pennsylvania. South Atlantic: Delaware,a District of Columbia, Florida, Georgia, Maryland, North Carolina, South Carolina, Virginia, and West Virginia. East North Central: Illinois, Indiana, Michigan, Ohio, and Wisconsin. West North Central: Iowa, Kansas, Minnesota, Missouri, Nebraska, North Dakota, and South Dakota. East South Central: Alabama,a Kentucky, Mississippi,a and Tennessee. West South Central: Arkansas, Louisiana, and Oklahoma, and Texas. Mountain: Arizona, Colorado, Idaho,a Montana, Nevada, New Mexico, Utah, and Wyoming. Pacific: Alaska,a California, Hawaii, Oregon, and Washington. aDid not contribute 2014 data.
References
-
- Prasad V, Rho J, Cifu A. The inferior vena cava filter: how could a medical device be so well accepted without any evidence of efficacy? JAMA Intern Med. 2013;173(7):493-495. - PubMed
-
- Stein PD, Kayali F, Olson RE. Twenty-one–year trends in the use of inferior vena cava filters. Arch Intern Med. 2004;164(14):1541-1545. - PubMed
-
- Moore PS, Andrews JS, Craven TE, et al. Trends in vena caval interruption. J Vasc Surg. 2010;52(1):118-125.e3. - PubMed
-
- PREPIC Study Group Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d’Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005;112(3):416-422. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
