

Self-administered Versus Directly Observed Once-Weekly Isoniazid and Rifapentine Treatment of Latent Tuberculosis Infection: A Randomized Trial
- PMID: 29114781
- PMCID: PMC5766341
- DOI: 10.7326/M17-1150
Self-administered Versus Directly Observed Once-Weekly Isoniazid and Rifapentine Treatment of Latent Tuberculosis Infection: A Randomized Trial
Abstract
Background: Expanding latent tuberculosis treatment is important to decrease active disease globally. Once-weekly isoniazid and rifapentine for 12 doses is effective but limited by requiring direct observation.
Objective: To compare treatment completion and safety of once-weekly isoniazid and rifapentine by self-administration versus direct observation.
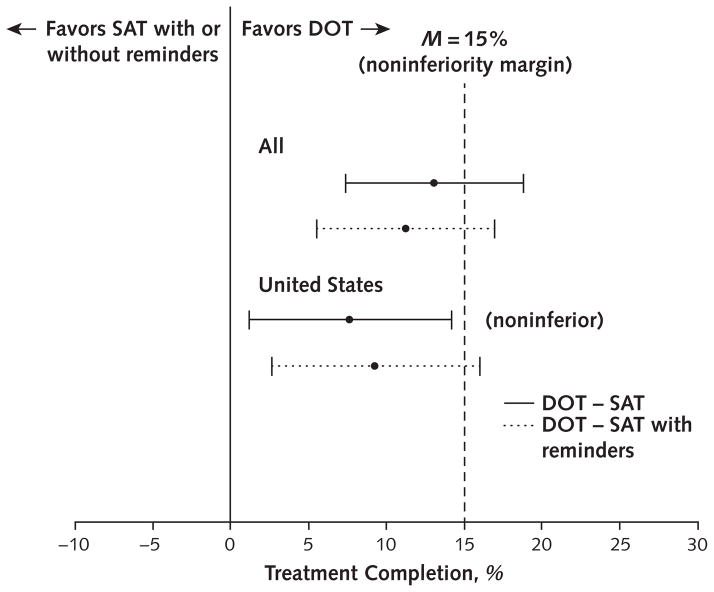
Design: An open-label, phase 4 randomized clinical trial designed as a noninferiority study with a 15% margin. Seventy-five percent or more of study patients were enrolled from the United States for a prespecified subgroup analysis. (ClinicalTrials.gov: NCT01582711).
Setting: Outpatient tuberculosis clinics in the United States, Spain, Hong Kong, and South Africa.
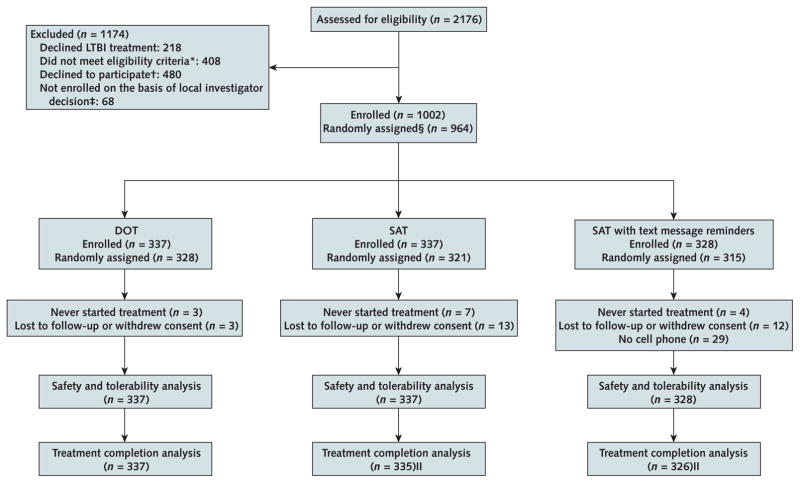
Participants: 1002 adults (aged ≥18 years) recommended for treatment of latent tuberculosis infection.
Intervention: Participants received once-weekly isoniazid and rifapentine by direct observation, self-administration with monthly monitoring, or self-administration with weekly text message reminders and monthly monitoring.
Measurements: The primary outcome was treatment completion, defined as 11 or more doses within 16 weeks and measured using clinical documentation and pill counts for direct observation, and self-reports, pill counts, and medication event-monitoring devices for self-administration. The main secondary outcome was adverse events.
Results: Median age was 36 years, 48% of participants were women, and 77% were enrolled at the U.S. sites. Treatment completion was 87.2% (95% CI, 83.1% to 90.5%) in the direct-observation group, 74.0% (CI, 68.9% to 78.6%) in the self-administration group, and 76.4% (CI, 71.3% to 80.8%) in the self-administration-with-reminders group. In the United States, treatment completion was 85.4% (CI, 80.4% to 89.4%), 77.9% (CI, 72.7% to 82.6%), and 76.7% (CI, 70.9% to 81.7%), respectively. Self-administered therapy without reminders was noninferior to direct observation in the United States; no other comparisons met noninferiority criteria. A few drug-related adverse events occurred and were similar across groups.
Limitation: Persons with latent tuberculosis infection enrolled in South Africa would not routinely be treated programmatically.
Conclusion: These results support using self-administered, once-weekly isoniazid and rifapentine to treat latent tuberculosis infection in the United States, and such treatment could be considered in similar settings when direct observation is not feasible.
Primary funding source: Centers for Disease Control and Prevention.
Figures
Comment in
-
Tailoring Treatment of Latent Tuberculosis to the Needs of Patients and Families.Ann Intern Med. 2017 Nov 21;167(10):742-743. doi: 10.7326/M17-2639. Epub 2017 Nov 7. Ann Intern Med. 2017. PMID: 29114744 No abstract available.
References
-
- Bibbins-Domingo K, Grossman DC, Curry SJ, Bauman L, Davidson KW, Epling JW, Jr, et al. US Preventive Services Task Force. Screening for latent tuberculosis infection in adults: US Preventive Services Task Force recommendation statement. JAMA. 2016;316:962–9. doi: 10.1001/jama.2016.11046. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous