

Factors Associated With Increases in US Health Care Spending, 1996-2013
- PMID: 29114831
- PMCID: PMC5818797
- DOI: 10.1001/jama.2017.15927
Factors Associated With Increases in US Health Care Spending, 1996-2013
Abstract
Importance: Health care spending in the United States increased substantially from 1995 to 2015 and comprised 17.8% of the economy in 2015. Understanding the relationship between known factors and spending increases over time could inform policy efforts to contain future spending growth.
Objective: To quantify changes in spending associated with 5 fundamental factors related to health care spending in the United States: population size, population age structure, disease prevalence or incidence, service utilization, and service price and intensity.
Design and setting: Data on the 5 factors from 1996 through 2013 were extracted for 155 health conditions, 36 age and sex groups, and 6 types of care from the Global Burden of Disease 2015 study and the Institute for Health Metrics and Evaluation's US Disease Expenditure 2013 project. Decomposition analysis was performed to estimate the association between changes in these factors and changes in health care spending and to estimate the variability across health conditions and types of care.
Exposures: Change in population size, population aging, disease prevalence or incidence, service utilization, or service price and intensity.
Main outcomes and measures: Change in health care spending from 1996 through 2013.
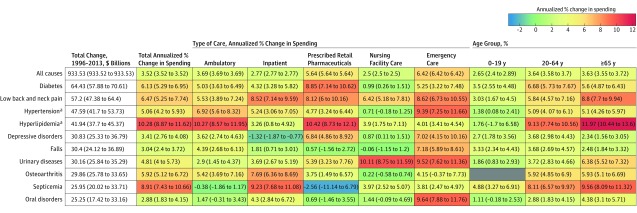
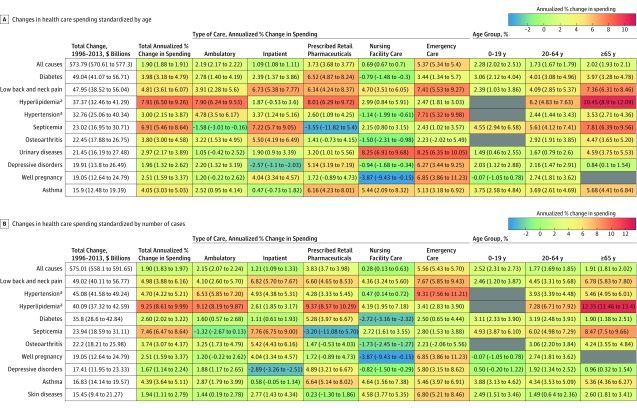
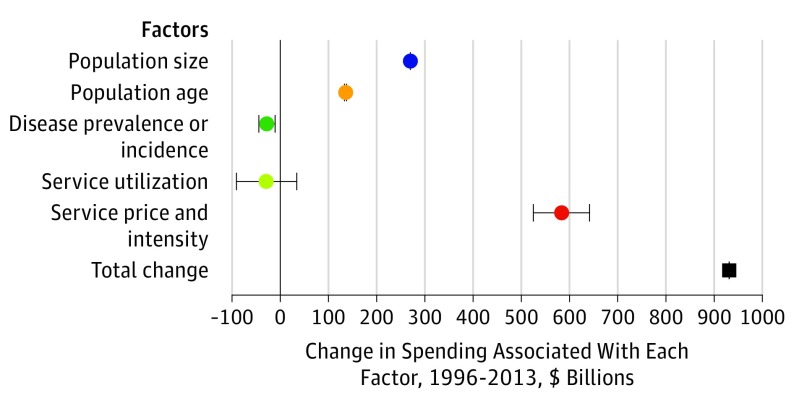
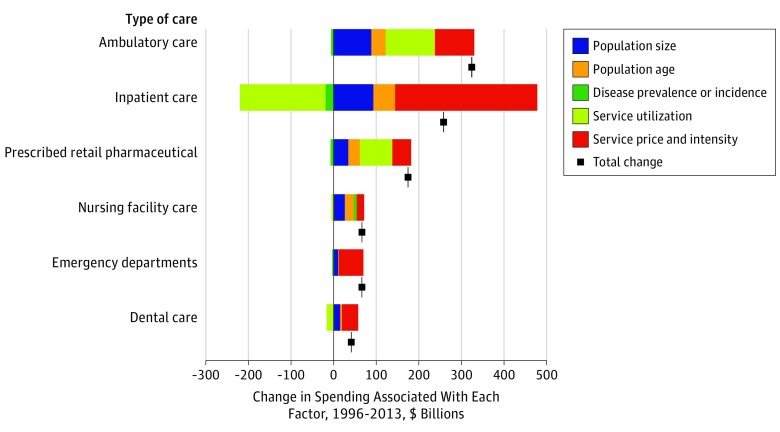
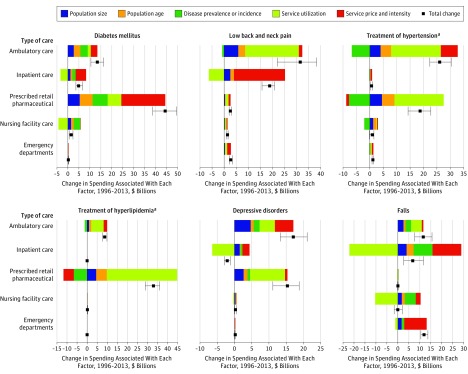
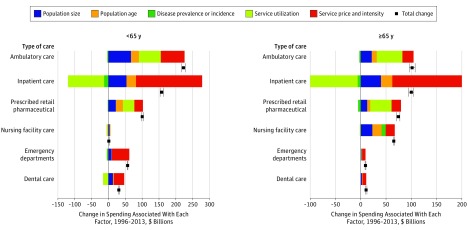
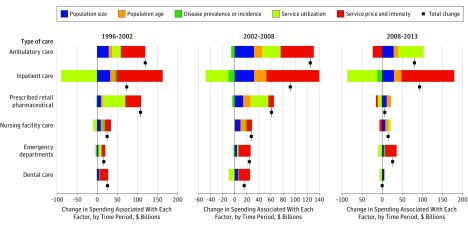
Results: After adjustments for price inflation, annual health care spending on inpatient, ambulatory, retail pharmaceutical, nursing facility, emergency department, and dental care increased by $933.5 billion between 1996 and 2013, from $1.2 trillion to $2.1 trillion. Increases in US population size were associated with a 23.1% (uncertainty interval [UI], 23.1%-23.1%), or $269.5 (UI, $269.0-$270.0) billion, spending increase; aging of the population was associated with an 11.6% (UI, 11.4%-11.8%), or $135.7 (UI, $133.3-$137.7) billion, spending increase. Changes in disease prevalence or incidence were associated with spending reductions of 2.4% (UI, 0.9%-3.8%), or $28.2 (UI, $10.5-$44.4) billion, whereas changes in service utilization were not associated with a statistically significant change in spending. Changes in service price and intensity were associated with a 50.0% (UI, 45.0%-55.0%), or $583.5 (UI, $525.2-$641.4) billion, spending increase. The influence of these 5 factors varied by health condition and type of care. For example, the increase in annual diabetes spending between 1996 and 2013 was $64.4 (UI, $57.9-$70.6) billion; $44.4 (UI, $38.7-$49.6) billion of this increase was pharmaceutical spending.
Conclusions and relevance: Increases in US health care spending from 1996 through 2013 were largely related to increases in health care service price and intensity but were also positively associated with population growth and aging and negatively associated with disease prevalence or incidence. Understanding these factors and their variability across health conditions and types of care may inform policy efforts to contain health care spending.
Conflict of interest statement
Figures
Comment in
-
Factors Associated With Increased US Health Care Spending: Implications for Controlling Health Care Costs.JAMA. 2017 Nov 7;318(17):1657-1658. doi: 10.1001/jama.2017.16802. JAMA. 2017. PMID: 29114814 No abstract available.
References
-
- Centers for Medicare & Medicaid Services National health expenditure data. https://www.cms.gov/research-statistics-data-and-systems/statistics-tren.... Accessed February 1, 2017.
-
- Bureau of Economic Analysis National economic accounts. https://www.bea.gov/national/. 2017. Accessed March 8, 2017.
-
- Emanuel E, Tanden N, Altman S, et al. A systemic approach to containing health care spending. N Engl J Med. 2012;367(10):949-954. - PubMed
-
- Starr M, Dominiak L, Aizcorbe A. Decomposing growth in spending finds annual cost of treatment contributed most to spending growth, 1980-2006. Health Aff (Millwood). 2014;33(5):823-831. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
