

Association Between Use of Thiopurines or Tumor Necrosis Factor Antagonists Alone or in Combination and Risk of Lymphoma in Patients With Inflammatory Bowel Disease
- PMID: 29114832
- PMCID: PMC5818785
- DOI: 10.1001/jama.2017.16071
Association Between Use of Thiopurines or Tumor Necrosis Factor Antagonists Alone or in Combination and Risk of Lymphoma in Patients With Inflammatory Bowel Disease
Abstract
Importance: An increased risk of lymphoma has been reported among patients receiving thiopurines for inflammatory bowel disease (IBD). The risk of lymphoma associated with anti-tumor necrosis factor (TNF) agents either alone or in combination with thiopurines is uncertain.
Objective: To assess the risk of lymphoma associated with thiopurines and anti-TNF agents, used alone or in combination, for the management of IBD.
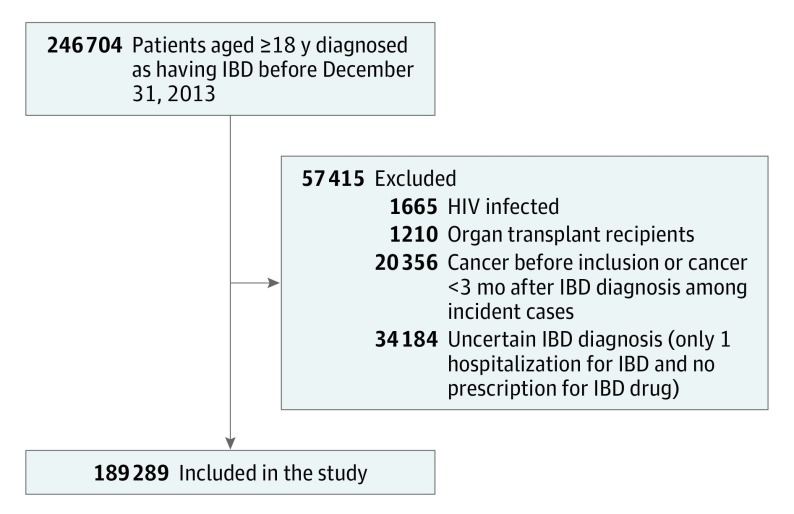
Design, setting, and participants: Nationwide cohort study based on French National Health Insurance databases. Patients aged 18 years or older identified with IBD were included from January 1, 2009, through December 31, 2013, and followed up until December 31, 2015.
Exposures: At each time of the follow-up, patients were categorized as being exposed to thiopurine monotherapy, anti-TNF monotherapy, or combination therapy, or being unexposed.
Main outcomes and measures: The primary outcome was incident lymphoma.
Results: Among the 189 289 patients included (54% women; median age, 43 years [interquartile range, 32-56 years]) and followed up for a median of 6.7 years, 123 069 were never exposed during follow-up, 50 405 were exposed to thiopurine monotherapy, 30 294 to anti-TNF monotherapy, and 14 229 to combination therapy. Overall, 336 lymphoma cases occurred: 220 in unexposed patients (incidence rate [IR] per 1000 person-years, 0.26; 95% CI, 0.23-0.29), 70 in patients exposed to thiopurine monotherapy (IR, 0.54; 95% CI, 0.41-0.67), 32 in patients exposed to anti-TNF monotherapy (IR, 0.41; 95% CI, 0.27-0.55), and 14 in patients exposed to combination therapy (IR, 0.95; 95% CI, 0.45-1.45). In a multivariable Cox model, compared with unexposed patients, the risk of lymphoma was higher among those exposed to thiopurine monotherapy (adjusted hazard ratio [aHR], 2.60; 95% CI, 1.96-3.44; P < .001), anti-TNF monotherapy (aHR, 2.41; 95% CI, 1.60-3.64; P < .001), or combination therapy (aHR, 6.11; 95% CI, 3.46-10.8; P < .001). The risk was higher in patients exposed to combination therapy vs those exposed to thiopurine monotherapy (aHR, 2.35; 95% CI, 1.31-4.22; P < .001) or anti-TNF monotherapy (aHR, 2.53; 95% CI, 1.35-4.77; P < .001).
Conclusions and relevance: Among adults with IBD, the use of thiopurine monotherapy or anti-TNF monotherapy was associated with a small but statistically significant increased risk of lymphoma compared with exposure to neither medication, and this risk was higher with combination therapy than with each of these treatments used alone. These findings may inform decisions regarding the benefits and risks of treatment.
Conflict of interest statement
Figures
References
-
- Colombel JF, Sandborn WJ, Reinisch W, et al. ; SONIC Study Group . Infliximab, azathioprine, or combination therapy for Crohn’s disease. N Engl J Med. 2010;362(15):1383-1395. - PubMed
-
- Reinisch W, Sandborn WJ, Hommes DW, et al. Adalimumab for induction of clinical remission in moderately to severely active ulcerative colitis: results of a randomised controlled trial. Gut. 2011;60(6):780-787. - PubMed
-
- Rutgeerts P, Van Assche G, Sandborn WJ, et al. ; EXTEND Investigators . Adalimumab induces and maintains mucosal healing in patients with Crohn’s disease: data from the EXTEND trial. Gastroenterology. 2012;142(5):1102-1111.e2. - PubMed
-
- D’Haens G, Baert F, van Assche G, et al. ; Belgian Inflammatory Bowel Disease Research Group; North-Holland Gut Club . Early combined immunosuppression or conventional management in patients with newly diagnosed Crohn’s disease: an open randomised trial. Lancet. 2008;371(9613):660-667. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
