

Hyperglycaemia induced by chronic i.p. and oral glucose loading leads to hypertension through increased Na+ retention in proximal tubule
- PMID: 29114945
- PMCID: PMC5794570
- DOI: 10.1113/EP086604
Hyperglycaemia induced by chronic i.p. and oral glucose loading leads to hypertension through increased Na+ retention in proximal tubule
Abstract
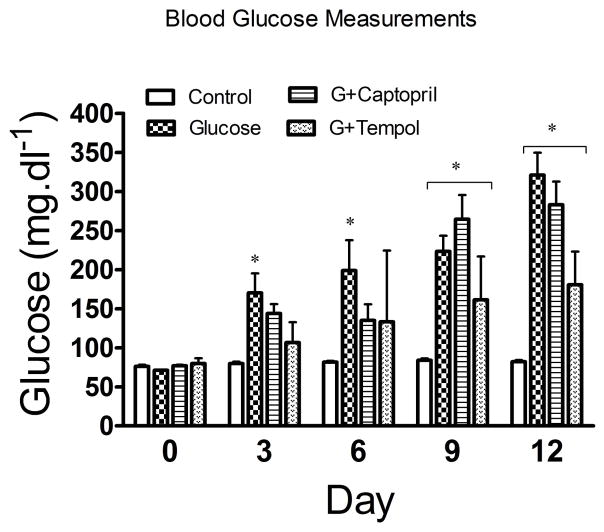
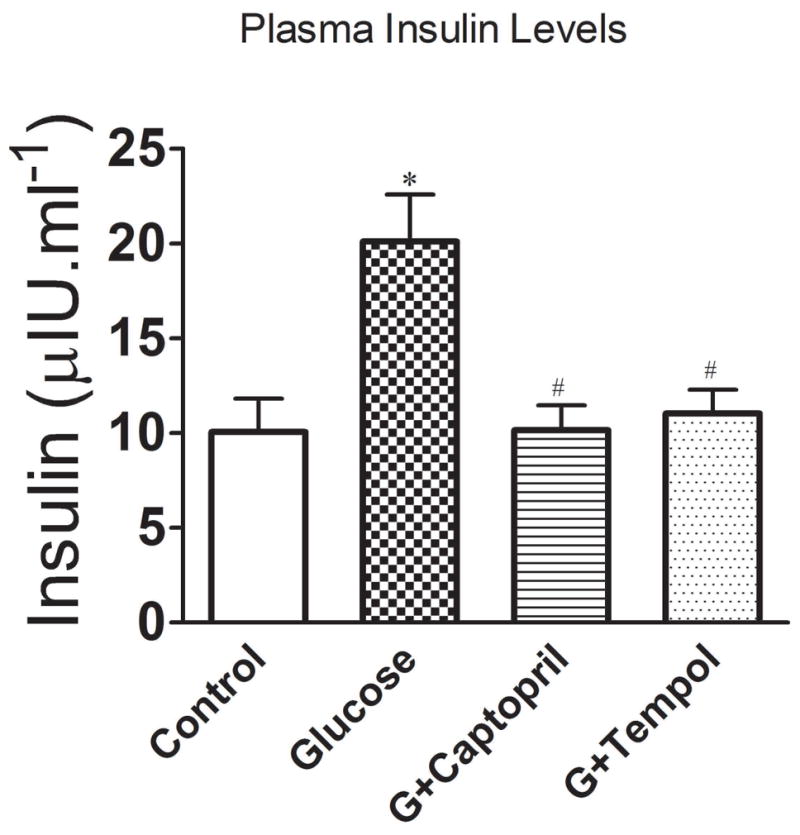
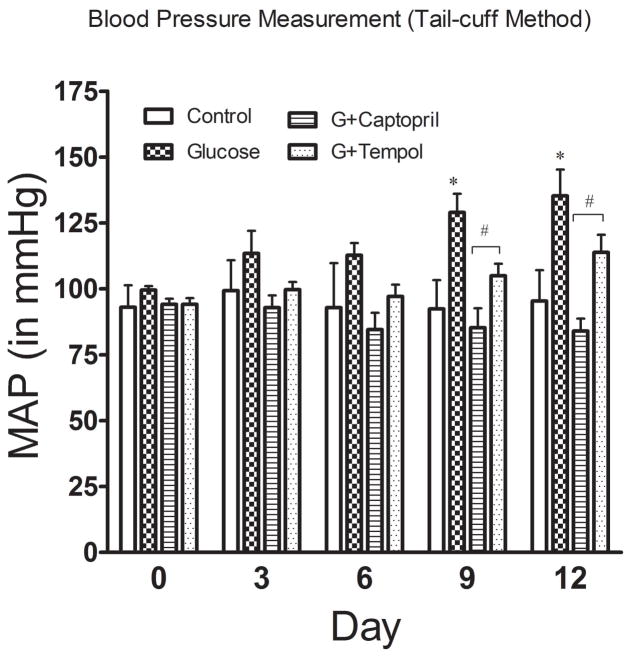
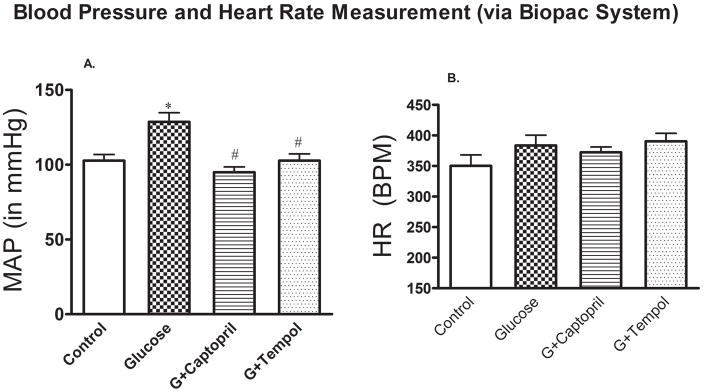
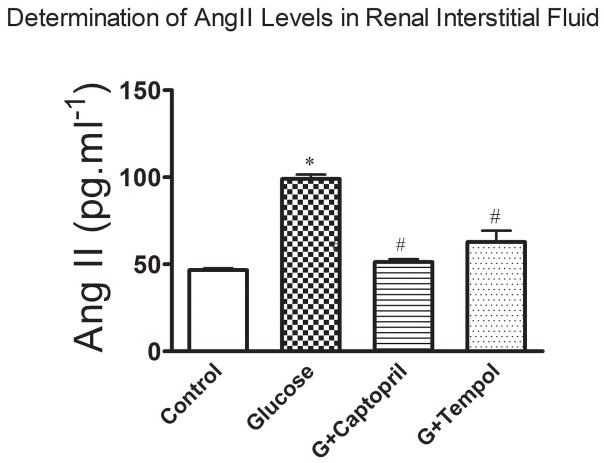
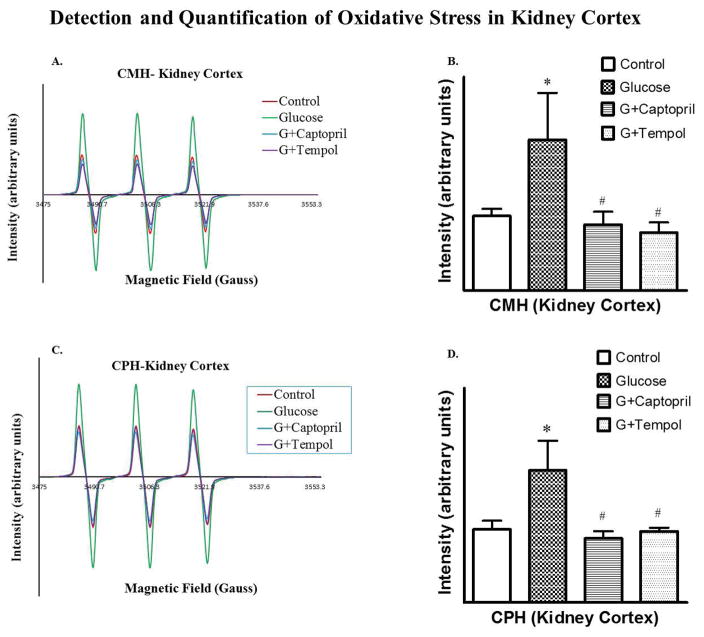
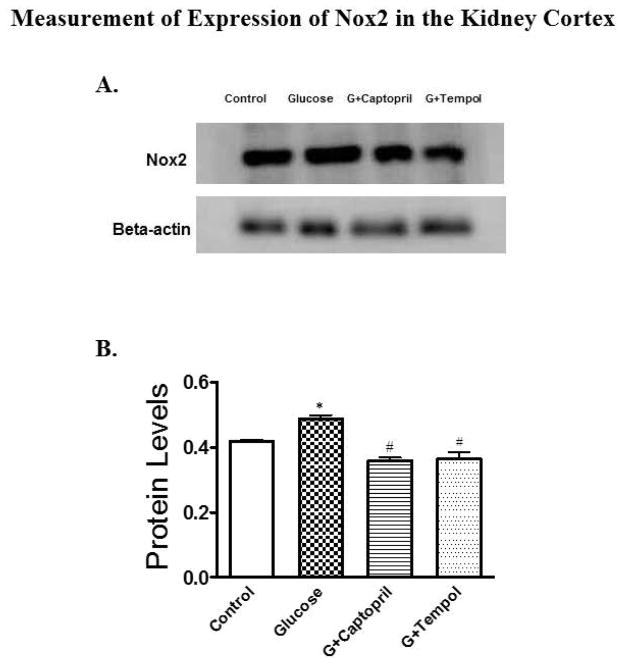
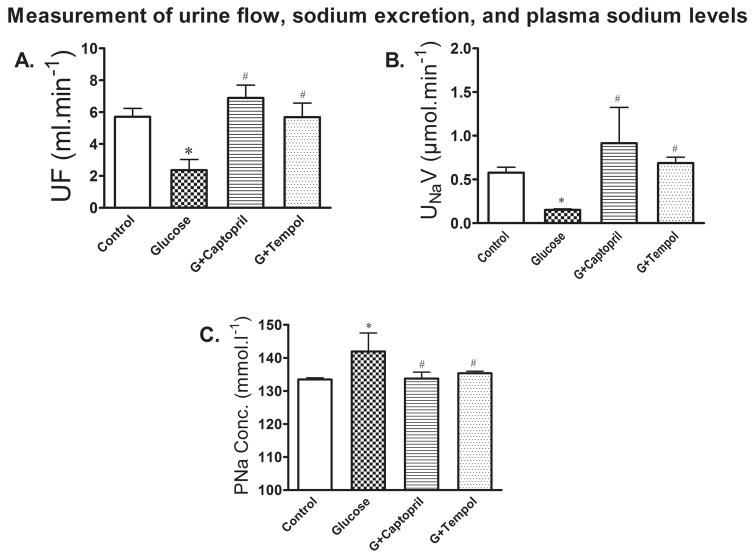
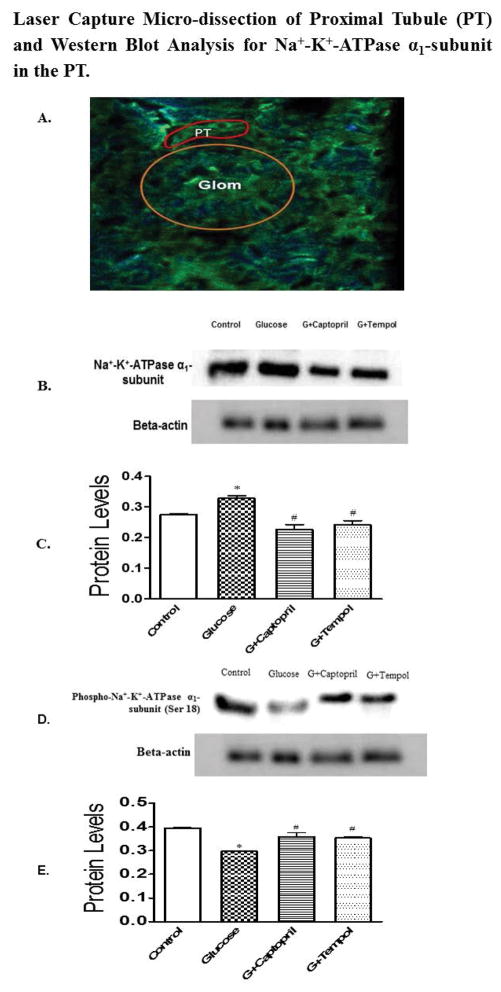
What is the central question of the study? Chronic glucose feeding accompanied by glucose injection (i.p.) causes sustained hyperglycaemia and hypertension in rats. The exact reason for the hypertension is not known. We explore some molecular pathways of the renal proximal tubule that might promote Na+ retention. What is the main finding and its importance? Development of hypertension was mediated by upregulation of the renal renin-angiotensin system and oxidative stress, acting via the Na+ -K+ -ATPase α1 -subunit in the proximal tubule, which appears to pump intracellular Na+ into the extracellular space, increasing Na+ reabsorption and blood pressure. Targeting the Na+ -K+ -ATPase α1 -subunit might provide a therapeutic strategy for treatment of hypertension. Feeding animals glucose-, fructose-, sucrose- and fat-enriched diets can lead to diet-induced hyperglycaemia, the severity of which largely depends on the types and concentrations of the nutrients used and duration of the dietary intervention. As a dietary intervention strategy, we adopted glucose-enriched diet and drinking water, with i.p. glucose injection at a dose previously determined to be effective to establish a sustained hyperglycaemia over a period of 2 weeks. We used four groups of Sprague-Dawley rats: control; glucose treated; glucose plus tempol treated; and glucose plus captopril treated. Blood glucose concentrations started to increase gradually from day 3, peaked (321 mg dl-1 ) at day 12 and remained at similar levels until the end of the study on day 14 in the glucose treated-group compared with the control group. In contrast, the tempol- and captopril-treated groups showed significantly high glucose concentrations only in the second week. The plasma insulin concentration was significantly increased in glucose-treated animals but not in tempol- and captopril-treated groups when compared with the control rats. We also observed elevated blood pressure in the glucose-treated group compared with the control group, which can be attributed to the increase in angiotensin II concentrations from 46.67 to 99 pg ml-1 (control versus glucose), increased oxidative stress in the cortical proximal tubule (PT), decreased urine flow, and increased expression and activity of the PT-specific α1 -subunit of Na+ -K+ -ATPase in the renal cortex, which is responsible for increased sodium reabsorption from epithelial cells of PT into the peritubular capillaries, leading to increased blood volume and eventual blood pressure. All these events were reversed in captopril- and tempol-treated animals.
Keywords: hyperglycemia; hypertension; renin-angiotensin system.
Published 2017. This article is a U.S. Government work and is in the public domain in the USA.
Conflict of interest statement
The authors declare no conflicts of interests
Figures
References
-
- Alanazi W, Fakhruddin S, Jackson KE. Microdialysis sampling of renal interstitial fluid in acute studies. International Journal of Biology. 2016;8:69–79.
-
- Banday AA, Lokhandwala MF. Loss of biphasic effect on Na/K-ATPase activity by angiotensin II involves defective angiotensin type 1 receptor-nitric oxide signaling. Hypertension. 2008;52:1099–1105. - PubMed
-
- Banday AA, Lokhandwala MF. Oxidative stress causes renal angiotensin II type 1 receptor upregulation, Na+/H+ exchanger 3 overstimulation, and hypertension. Hypertension. 2011;57:452–459. - PubMed
-
- Brezniceanu ML, Liu F, Wei CC, Tran S, Schetelli S, Zhang SL, Guo DF, Filep JG, Ingelfinger JR, Chan JS. Catalase overexpression attenuates angiotensinogen expression and apoptosis in diabetic mice. Kidney Int. 2007;71:912–923. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials