

Venovenous extracorporeal membrane oxygenation devices-related colonisations and infections
- PMID: 29116464
- PMCID: PMC5676570
- DOI: 10.1186/s13613-017-0335-9
Venovenous extracorporeal membrane oxygenation devices-related colonisations and infections
Abstract
Background: Nosocomial infections occurring during extracorporeal membrane oxygenation (ECMO) support have already been reported, but few studied infections directly related to ECMO devices. This study aims to evaluate the rate of both colonisations and infections related to ECMO devices at the time of ECMO removal.
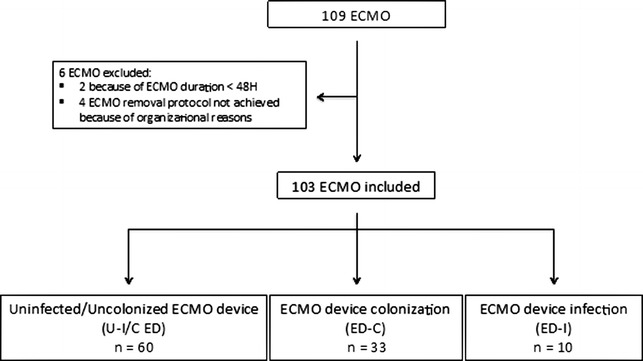
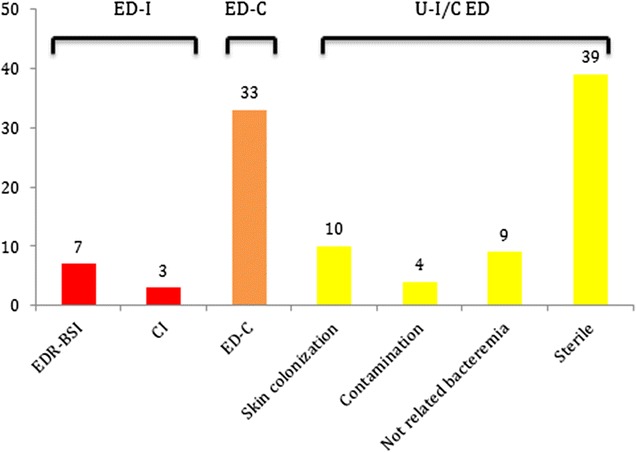
Results: We included all consecutive adult patients treated with venovenous ECMO (VV-ECMO) for at least 48 h during a 34-month study. At the time of ECMO removal, blood cultures, swab cultures on insertion cannula site and intravascular cannula extremity cultures were systematically performed. Each ECMO device was classified according to the infectious status into three groups: (1) uninfected/uncolonised ECMO device, (2) ECMO device colonisation and (3) ECMO device infection. Ninety-nine patients underwent 103 VV-ECMO, representing 1472 ECMO days. The ECMO device infection rate was 9.7% (10 events), including 7 ECMO device-related bloodstream infections (6.8%). The ECMO device colonisation rate was 32% (33 events). No difference was observed between the three groups, regarding days of mechanical ventilation, ICU length of stay, ICU mortality and in-hospital mortality. We observed a longer ECMO duration in the ECMO device colonisation group as compared to the uninfected/uncolonised ECMO device group [12 (9-20 days) vs. 5 days (5-16 days), respectively, p < 0.05].
Conclusions: At the time of ECMO removal, systematic blood culture and intravascular extremity cannula culture may help to diagnose ECMO device-related infection. We reported a quite low infection rate related to ECMO device. Further studies are needed to evaluate the benefits of systematic strategies of cannula culture at the time of ECMO removal.
Keywords: Colonisation rate; Device-related colonisation; Device-related infections; Infection rate; Venovenous extracorporeal membrane oxygenation.
Figures
Comment in
-
Infection and colonisation in V-V ECMO-not a predictor of poor outcome.J Thorac Dis. 2018 Jun;10(Suppl 17):S2045-S2047. doi: 10.21037/jtd.2018.05.128. J Thorac Dis. 2018. PMID: 30023114 Free PMC article. No abstract available.
References
-
- Rehder KJ, Turner DA, Cheifetz IM. Extracorporeal membrane oxygenation for neonatal and pediatric respiratory failure: an evidence-based review of the past decade (2002–2012) Pediatr Crit Care Med J Soc Crit Care Med World Fed Pediatr Intensive Crit Care Soc. 2013;14:851–861. - PubMed
-
- Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators. Extracorporeal Membrane Oxygenation for 2009 Influenza A(H1N1) Acute Respiratory Distress Syndrome. JAMA. 2009; 302:1888–1895; 10.1001/jama.2009.1535. - PubMed
-
- Camboni D, Philipp A, Lubnow M, Bein T, Haneya A, Diez C, Schmid C, Müller T. Support time-dependent outcome analysis for veno-venous extracorporeal membrane oxygenation. Eur J Cardio Thorac Surg Off J Eur Assoc Cardio Thorac Surg. 2011;40:1341-1346-1347. - PubMed
-
- Roch A, Hraiech S, Masson E, Grisoli D, Forel J-M, Boucekine M, Morera P, Guervilly C, Adda M, Dizier S, Toesca R, Collart F, Papazian L. Outcome of acute respiratory distress syndrome patients treated with extracorporeal membrane oxygenation and brought to a referral center. Intensive Care Med. 2014;40:74–83. doi: 10.1007/s00134-013-3135-1. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
