

Worse Outcome in Stroke Patients Treated with rt-PA Without Early Reperfusion: Associated Factors
- PMID: 29116527
- PMCID: PMC6061244
- DOI: 10.1007/s12975-017-0584-9
Worse Outcome in Stroke Patients Treated with rt-PA Without Early Reperfusion: Associated Factors
Abstract
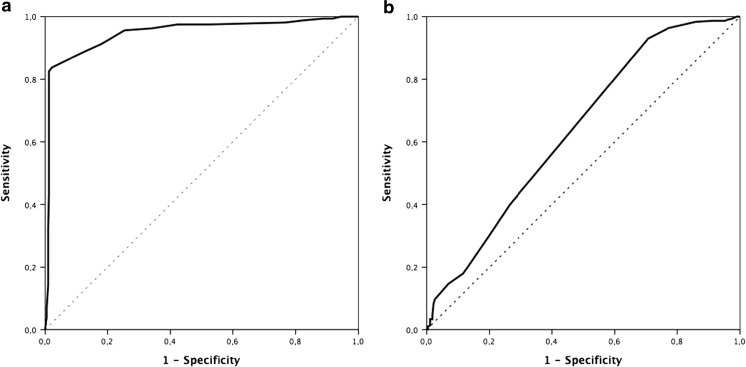
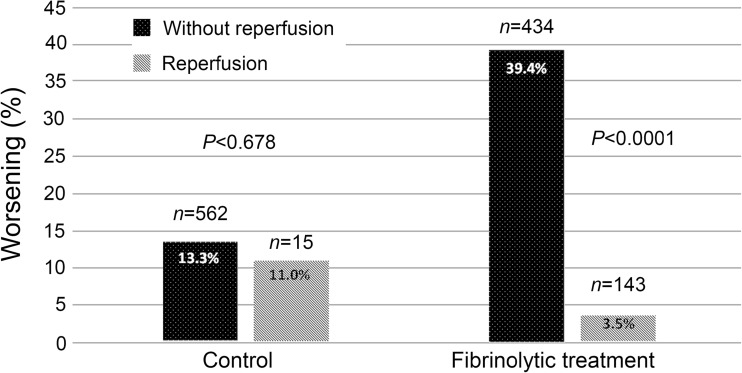
Based on preclinical studies suggesting that recombinant tissue plasminogen activator (rt-PA) may promote ischemic brain injuries, we investigated in patients the possible risk of worse clinical outcome after rt-PA treatment as a result of its inability to resolve cerebral ischemia. Here, we designed a cohort study using a retrospective analysis of patients who received treatment with intravenous (4.5-h window) or intraarterial rt-PA, without or with thrombectomy. Controls were consecutive patients who did not receive recanalization treatment, who met all inclusion criteria. As a marker of reperfusion, we defined the variable of early neurological improvement as the difference between the score of the National Institute of Health Stroke Scale (NIHSS) (at admission and 24 h). The main variable was worsening of the patient's functional situation in the first 3 months. To compare quantitative variables, we used Student's t test or the Mann-Whitney test. To estimate the odds ratios of each independent variable in the patient's worsening in the first 3 months, we used a logistic regression model. We included 1154 patients; 577 received rt-PA, and 577 served as controls. In the group of patients treated with rt-PA, 39.4% who did not present clinical reperfusion data developed worsening within 3 months after stroke compared with 3.5% of patients with reperfusion (P < 0.0001). These differences were not significant in the control group. In summary, administration of rt-PA intravenously or intraarterially without reperfusion within the first 24 h may be associated with a higher risk of functional deterioration in the first 3 months.
Keywords: Blood-brain barrier; Critical care; Hemorrhage transformation; Ischemic stroke; Prognosis.
Conflict of interest statement
Conflict of Interest
The authors declare that they have no conflicts of interest.
Ethical Approval and Patient Consent
This research was carried out in accordance with the Declaration of Helsinki of the World Medical Association (2008) and approved by the Ethics Committee of the Servizo Galego de Saúde. Informed consent was obtained from each patient or their relatives after full explanation of the procedures.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
