

Effectiveness of Online Collaborative Care for Treating Mood and Anxiety Disorders in Primary Care: A Randomized Clinical Trial
- PMID: 29117275
- PMCID: PMC5833533
- DOI: 10.1001/jamapsychiatry.2017.3379
Effectiveness of Online Collaborative Care for Treating Mood and Anxiety Disorders in Primary Care: A Randomized Clinical Trial
Erratum in
-
Error in Figure 3.JAMA Psychiatry. 2018 Jan 1;75(1):104. doi: 10.1001/jamapsychiatry.2017.3977. JAMA Psychiatry. 2018. PMID: 29214282 Free PMC article. No abstract available.
Abstract
Importance: Collaborative care for depression and anxiety is superior to usual care from primary care physicians for these conditions; however, challenges limit its provision in routine practice and at scale. Advances in technology may overcome these barriers but have yet to be tested.
Objective: To examine the effectiveness of combining an internet support group (ISG) with an online computerized cognitive behavioral therapy (CCBT) provided via a collaborative care program for treating depression and anxiety vs CCBT alone and whether providing CCBT in this manner is more effective than usual care.
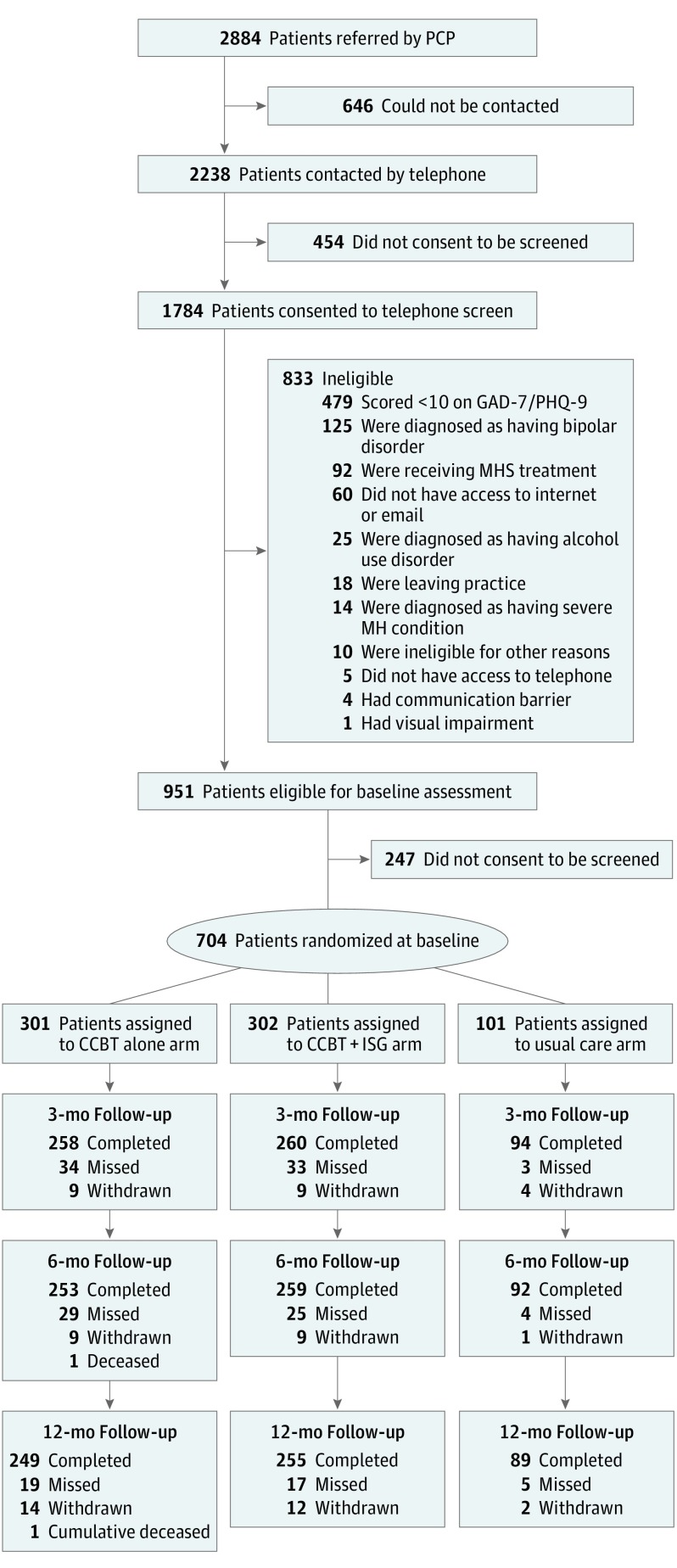
Design, setting, and participants: In this 3-arm randomized clinical trial with blinded outcome assessments, primary care physicians from 26 primary care practices in Pittsburgh, Pennsylvania, referred 2884 patients aged 18 to 75 years in response to an electronic medical record prompt from August 2012 to September 2014. Overall, 704 patients (24.4%) met all eligibility criteria and were randomized to CCBT alone (n = 301), CCBT+ISG (n = 302), or usual care (n = 101). Intent-to-treat analyses were conducted November 2015 to January 2017.
Interventions: Six months of guided access to an 8-session CCBT program provided by care managers who informed primary care physicians of their patients' progress and promoted patient engagement with our online programs.
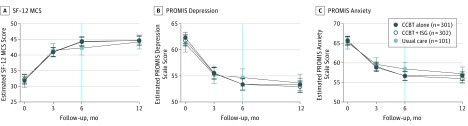
Main outcomes and measures: Mental health-related quality of life (12-Item Short-Form Health Survey Mental Health Composite Scale) and depression and anxiety symptoms (Patient-Reported Outcomes Measurement Information System) at 6-month follow-up, with treatment durability assessed 6 months later.
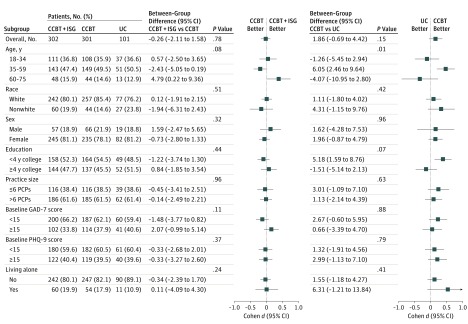
Results: Of the 704 randomized patients, 562 patients (79.8%) were female, and the mean (SD) age was 42.7 (14.3) years. A total of 604 patients (85.8%) completed our primary 6-month outcome assessment. At 6-month assessment, 254 of 301 patients (84.4%) receiving CCBT alone started the program (mean [SD] sessions completed, 5.4 [2.8]), and 228 of 302 patients (75.5%) in the CCBT+ISG cohort logged into the ISG at least once, of whom 141 (61.8%) provided 1 or more comments or posts (mean, 10.5; median [range], 3 [1-306]). Patients receiving CCBT+ISG reported similar 6-month improvements in mental health-related quality of life, mood, and anxiety symptoms compared with patients receiving CCBT alone. However, compared with patients receiving usual care, patients in the CCBT alone cohort reported significant 6-month effect size improvements in mood (effect size, 0.31; 95% CI, 0.09-0.53) and anxiety (effect size, 0.26; 95% CI, 0.05-0.48) that persisted 6 months later, and completing more CCBT sessions produced greater effect size improvements in mental health-related quality of life and symptoms.
Conclusions and relevance: While providing moderated access to an ISG provided no additional benefit over guided CCBT at improving mental health-related quality of life, mood, and anxiety symptoms, guided CCBT alone is more effective than usual care for these conditions.
Trial registration: clinicaltrials.gov Identifier: NCT01482806.
Conflict of interest statement
Figures
References
-
- Karyotaki E, Riper H, Twisk J, et al. . Efficacy of self-guided internet-based cognitive behavioral therapy in the treatment of depressive symptoms: a meta-analysis of individual participant data. JAMA Psychiatry. 2017;74(4):351-359. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
