

Intrapartum Antibiotic Chemoprophylaxis Policies for the Prevention of Group B Streptococcal Disease Worldwide: Systematic Review
- PMID: 29117324
- PMCID: PMC5850619
- DOI: 10.1093/cid/cix654
Intrapartum Antibiotic Chemoprophylaxis Policies for the Prevention of Group B Streptococcal Disease Worldwide: Systematic Review
Abstract
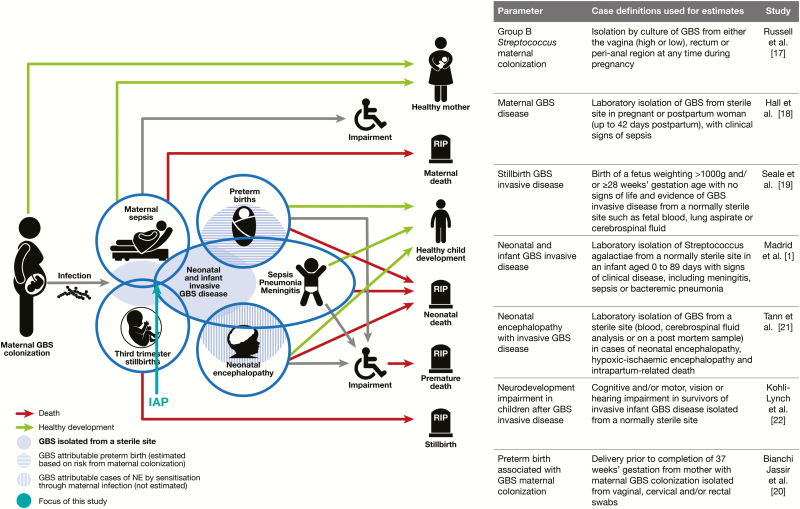
Background: Intrapartum antibiotic chemoprophylaxis (IAP) prevents most early-onset group B streptococcal (GBS) disease. However, there is no description of how IAP is used around the world. This article is the sixth in a series estimating the burden of GBS disease. Here we aimed to review GBS screening policies and IAP implementation worldwide.
Methods: We identified data through (1) systematic literature reviews (PubMed/Medline, Embase, Literature in the Health Sciences in Latin America and the Caribbean [LILACS], World Health Organization library database [WHOLIS], and Scopus) and unpublished data from professional societies and (2) an online survey and searches of policies from medical societies and professionals. We included data on whether an IAP policy was in use, and if so whether it was based on microbiological or clinical risk factors and how these were applied, as well as the estimated coverage (percentage of women receiving IAP where indicated).
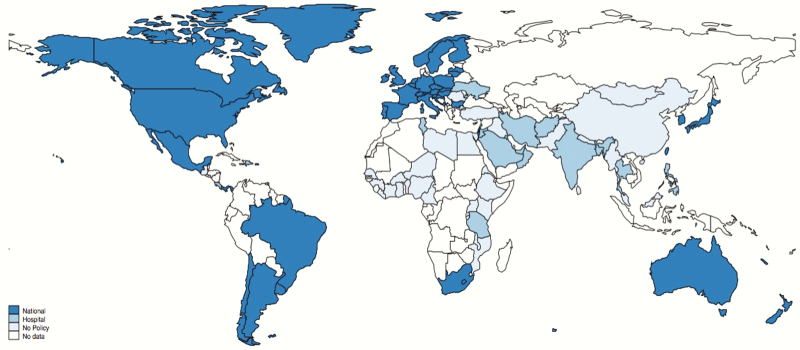
Results: We received policy information from 95 of 195 (49%) countries. Of these, 60 of 95 (63%) had an IAP policy; 35 of 60 (58%) used microbiological screening, 25 of 60 (42%) used clinical risk factors. Two of 15 (13%) low-income, 4 of 16 (25%) lower-middle-income, 14 of 20 (70%) upper-middle-income, and 40 of 44 (91%) high-income countries had any IAP policy. The remaining 35 of 95 (37%) had no national policy (25/33 from low-income and lower-middle-income countries). Coverage varied considerably; for microbiological screening, median coverage was 80% (range, 20%-95%); for clinical risk factor-based screening, coverage was 29% (range, 10%-50%). Although there were differences in the microbiological screening methods employed, the individual clinical risk factors used were similar.
Conclusions: There is considerable heterogeneity in IAP screening policies and coverage worldwide. Alternative global strategies, such as maternal vaccination, are needed to enhance the scope of global prevention of GBS disease.
Keywords: group B Streptococcus; intrapartum antibiotic chemoprophylaxis.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures



References
-
- Verani JR, McGee L, Schrag SJ; Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention (CDC) Prevention of perinatal group B streptococcal disease—revised guidelines from CDC, 2010. MMWR Recomm Rep 2010; 59:1–36. - PubMed
-
- Baltimore RS. Consequences of prophylaxis for group B streptococcal infections of the neonate. Semin Perinatol 2007; 31:33–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
