

The South African Tuberculosis Care Cascade: Estimated Losses and Methodological Challenges
- PMID: 29117342
- PMCID: PMC5853316
- DOI: 10.1093/infdis/jix335
The South African Tuberculosis Care Cascade: Estimated Losses and Methodological Challenges
Abstract
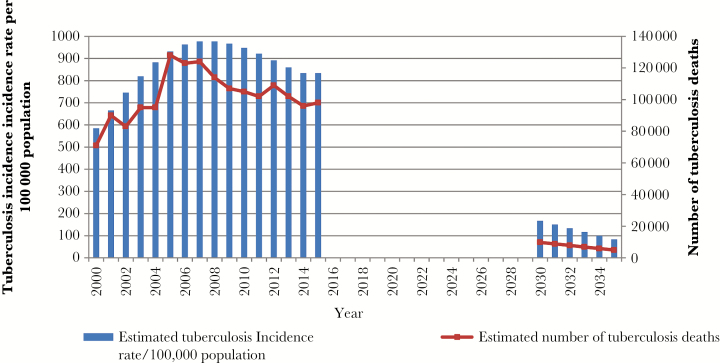
Background: While tuberculosis incidence and mortality are declining in South Africa, meeting the goals of the End TB Strategy requires an invigorated programmatic response informed by accurate data. Enumerating the losses at each step in the care cascade enables appropriate targeting of interventions and resources.
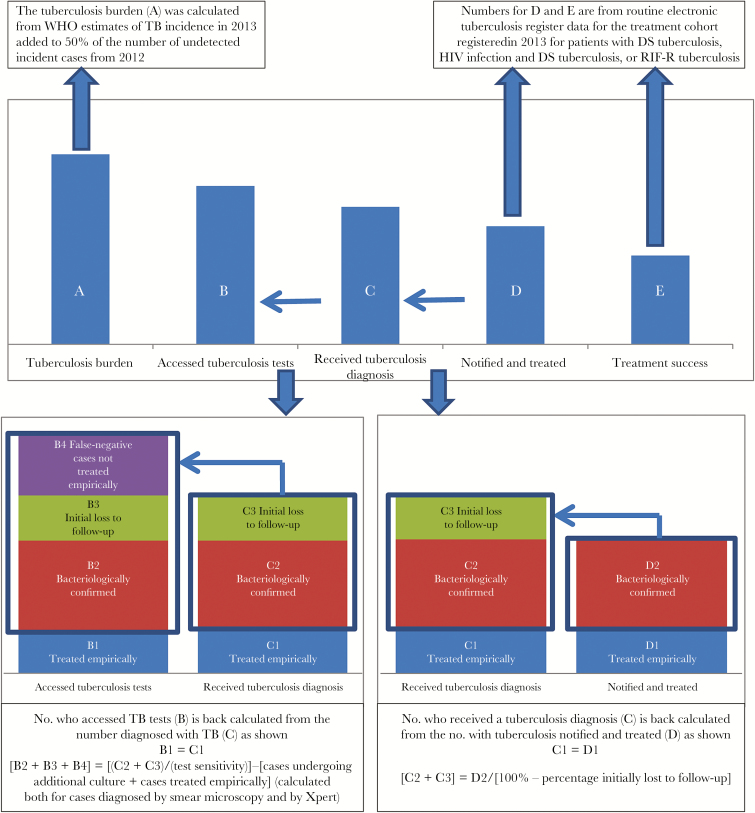
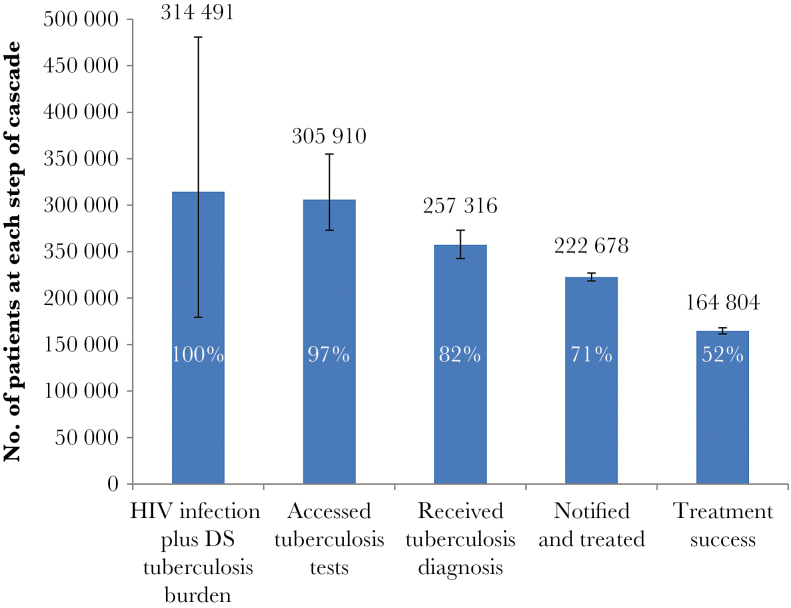
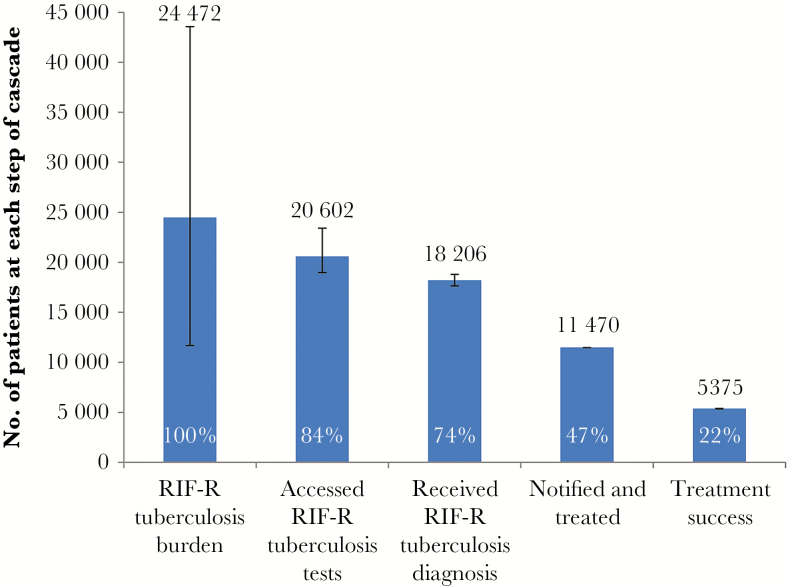
Methods: We estimated the tuberculosis burden; the number and proportion of individuals with tuberculosis who accessed tests, had tuberculosis diagnosed, initiated treatment, and successfully completed treatment for all tuberculosis cases, for those with drug-susceptible tuberculosis (including human immunodeficiency virus (HIV)-coinfected cases) and rifampicin-resistant tuberculosis. Estimates were derived from national electronic tuberculosis register data, laboratory data, and published studies.
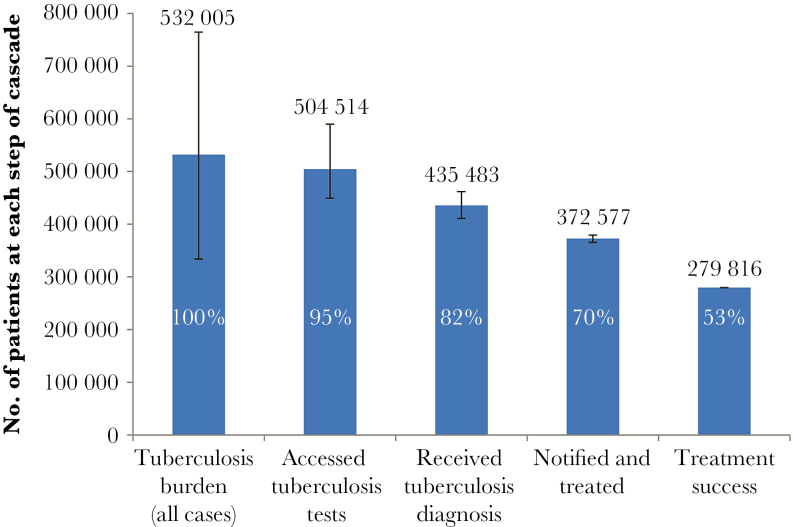
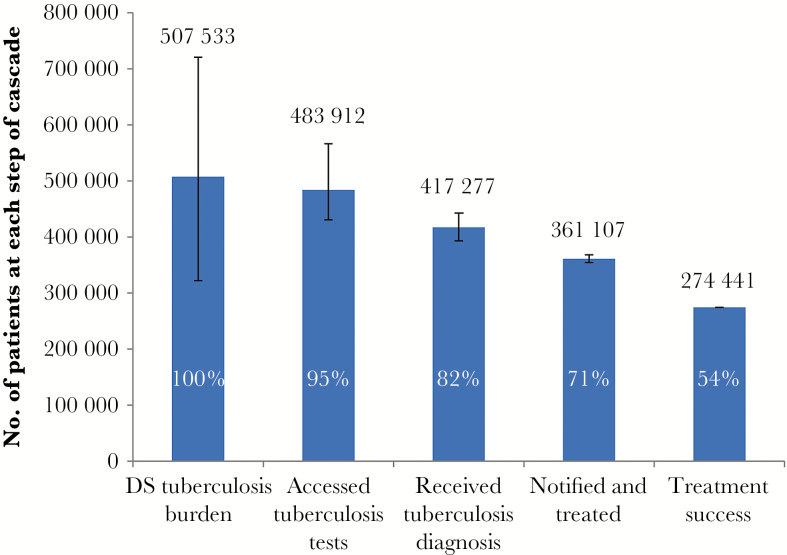
Results: The overall tuberculosis burden was estimated to be 532005 cases (range, 333760-764480 cases), with successful completion of treatment in 53% of cases. Losses occurred at multiple steps: 5% at test access, 13% at diagnosis, 12% at treatment initiation, and 17% at successful treatment completion. Overall losses were similar among all drug-susceptible cases and those with HIV coinfection (54% and 52%, respectively, successfully completed treatment). Losses were substantially higher among rifampicin- resistant cases, with only 22% successfully completing treatment.
Conclusion: Although the vast majority of individuals with tuberculosis engaged the public health system, just over half were successfully treated. Urgent efforts are required to improve implementation of existing policies and protocols to close gaps in tuberculosis diagnosis, treatment initiation, and successful treatment completion.
Keywords: Tuberculosis; care cascade; case-finding; continuum of care; initial loss to follow-up; treatment success.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- World Health Organization (WHO). Global tuberculosis report 2016. Geneva: WHO, 2016.
-
- South African National Institute for Communicable Diseases. South African tuberculosis drug-resistance survey 2012–14. Johannesburg, South Africa: National Institute for Communicable Diseases, 2016. Available at: http://www.nicd.ac.za/assets/files/K-12750%20NICD%20National%20Survey%20.... Accessed 22 July 2017.
-
- World Health Organization. The End TB Strategy. Geneva, Switzerland: WHO, 2015.
-
- WHO TB burden estimates Geneva, Switzerland: WHO, 2016. Available at: http://www.who.int/tb/country/data/download/en/. Accessed 26 October 2016.
-
- Bhardwaj S, Barron P, Pillay Y, et al. Elimination of mother-to-child transmission of HIV in South Africa: rapid scale-up using quality improvement. S Afr Med J 2014; 104:239–43. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
