

Delivering Patient-Centered Care in a Fragile State: Using Patient-Pathway Analysis to Understand Tuberculosis-Related Care Seeking in Pakistan
- PMID: 29117348
- PMCID: PMC5853661
- DOI: 10.1093/infdis/jix380
Delivering Patient-Centered Care in a Fragile State: Using Patient-Pathway Analysis to Understand Tuberculosis-Related Care Seeking in Pakistan
Abstract
Background: Pakistan has the sixth largest population in the world and boasts the fifth greatest burden of tuberculosis. The Government of Pakistan has set the ambitious goal of zero deaths due to tuberculosis and universal access to tuberculosis care by 2020. Successfully reaching these goals is dependent on the country's capacity to diagnose and successfully treat an estimated 200000 unnotified or missing patients with tuberculosis.
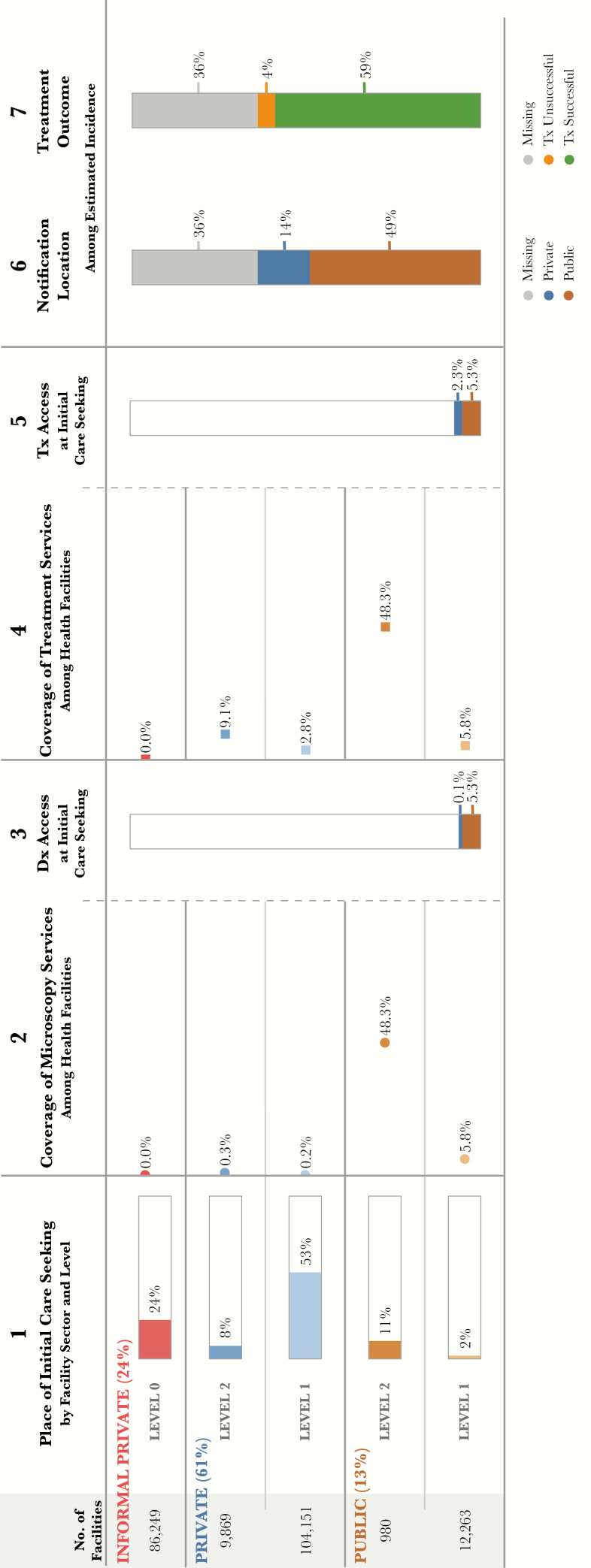
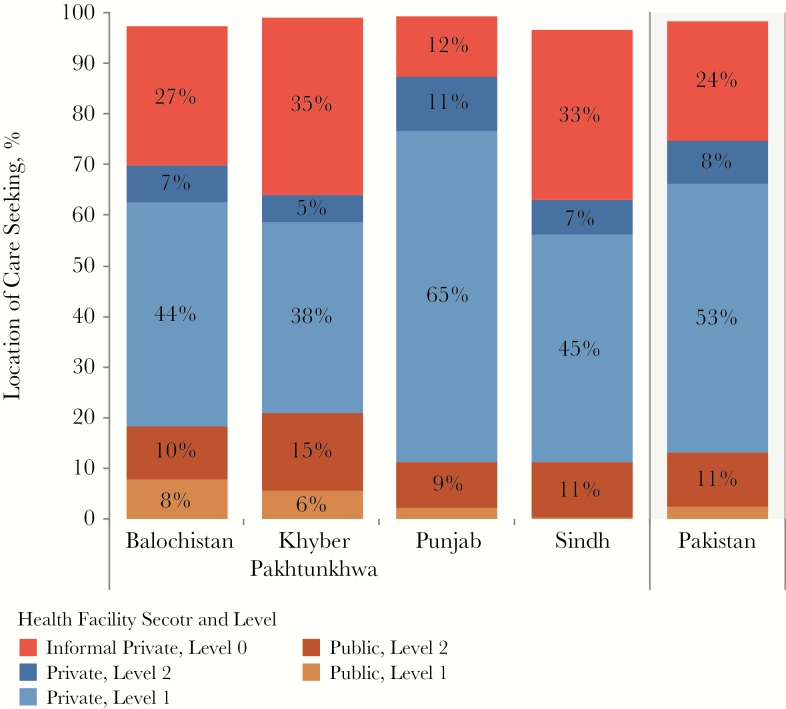
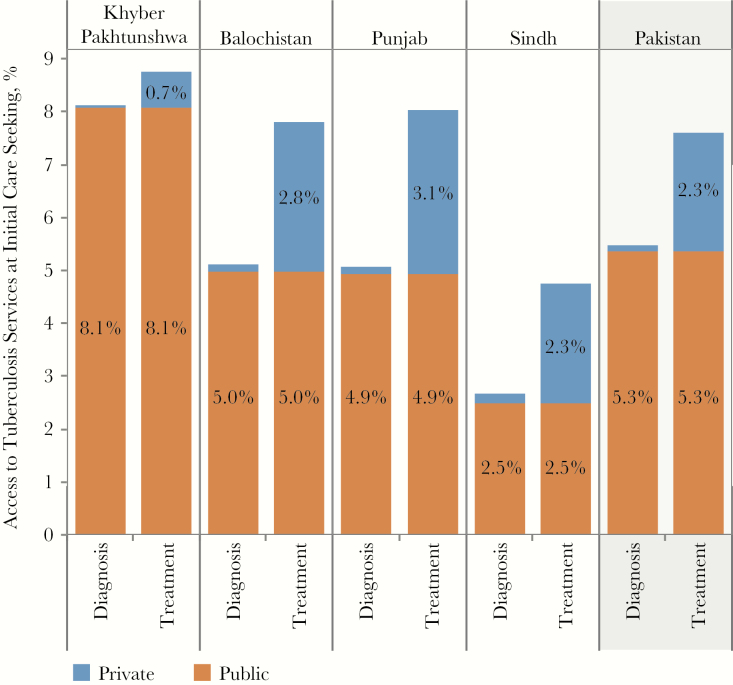
Methods: A patient-pathway analysis (PPA) was conducted at the national level, as well as for each of the 4 provinces, to assess the alignment between patient care seeking and the availability of tuberculosis diagnostic and treatment services.
Results: Almost 90% of patients initiated care in the private sector, which accounts for only 15% of facilities with the capacity for tuberculosis diagnosis and treatment. Across the country, nearly 50% of tuberculosis microscopy laboratories were located in public-sector-basic health units and regional health centers. However, very few patients initiated care in these facilities. Overall, tuberculosis case detection was high given the low likelihood of patients reaching facilities with the capacity for tuberculosis service delivery during their first visit.
Discussion: Improving the engagement of the informal sector and lower-level clinicians will improve the efficiency and timeliness of tuberculosis diagnosis for patients in Pakistan. Concurrently, the apparent strength of the referral networks connecting community-level workers and private clinicians to the public sector for tuberculosis diagnosis and treatment suggests that strengthening the capacity of the public sector could be valuable.
Keywords: Tuberculosis; care seeking; case notification; diagnostic; patient-pathway analysis; private; public.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- World Bank. Population, total. 2015 http://data.worldbank.org/indicator/SP.POP.TOTL?locations=PK&year_high_d.... Accessed 7 May 2017.
-
- World Bank. Rural population (% of total population). 2015 http://data.worldbank.org/indicator/SP.RUR.TOTL.ZS?locations=PK.
-
- Fund for Peace. Fragile states index 2016 http://reliefweb.int/report/world/fragile-states-index-2016.
-
- Ministry of National Health Services Regulations and Coordination. Pakistan 2025: one nation–one vision 2014. http://fics.seecs.edu.pk/Vision/Vision-2025/Pakistan-Vision-2025.pdf.
-
- Institute for Health Metrics and Evaluation. Pakistan. 2015 http://www.healthdata.org/pakistan. Accessed 7 May 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
