

Finding the Missing Patients With Tuberculosis: Lessons Learned From Patient-Pathway Analyses in 5 Countries
- PMID: 29117351
- PMCID: PMC5853970
- DOI: 10.1093/infdis/jix388
Finding the Missing Patients With Tuberculosis: Lessons Learned From Patient-Pathway Analyses in 5 Countries
Abstract
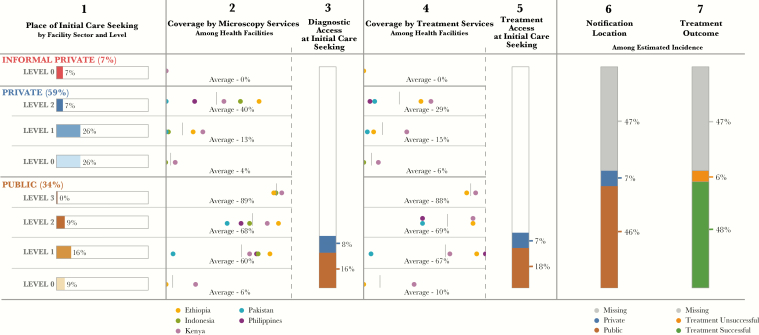
Background: Despite significant progress in diagnosis and treatment of tuberculosis over the past 2 decades, millions of patients with tuberculosis go unreported every year. The patient-pathway analysis (PPA) is designed to assess the alignment between tuberculosis care-seeking patterns and the availability of tuberculosis services. The PPA can help programs understand where they might find the missing patients with tuberculosis.
Methods: This analysis aggregates and compares the PPAs from case studies in Kenya, Ethiopia, Indonesia, the Philippines, and Pakistan.
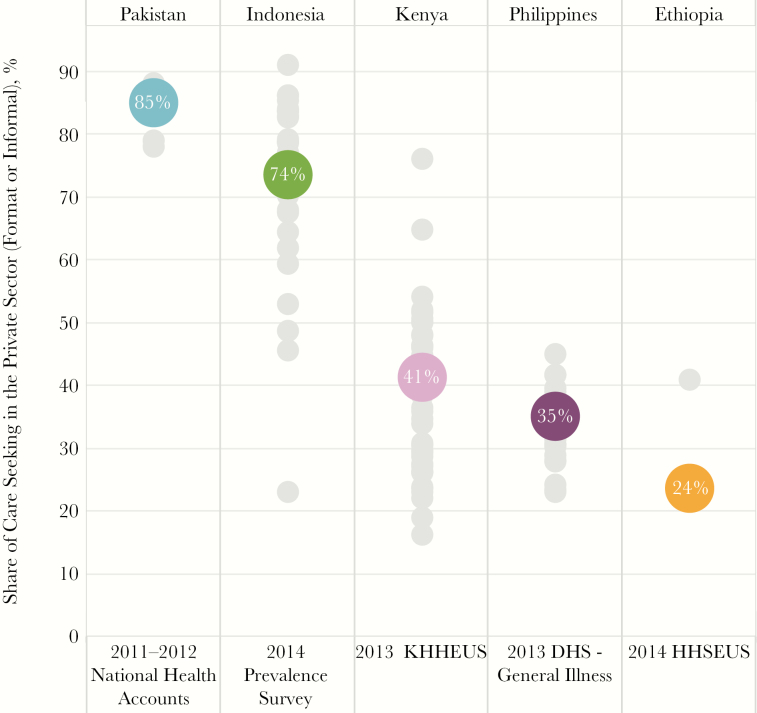
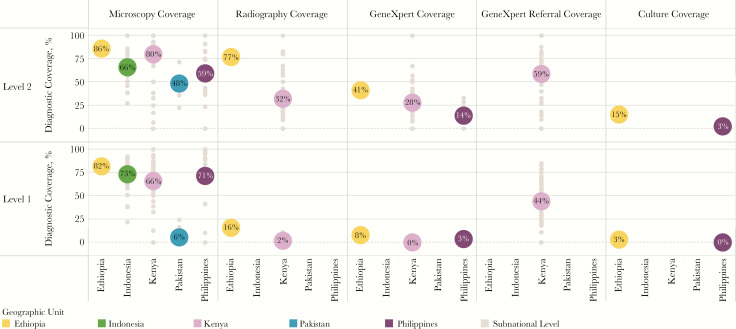
Results: Across the 5 countries, 24% of patients with tuberculosis initiated care seeking in a facility with tuberculosis diagnostic capacity. Forty-two percent of patients sought care at level 0 facilities, where there was generally no tuberculosis diagnostic capacity; another 42% of patients sought care at level 1 facilities, of which 39% had diagnostic capacity. Sixty-six percent of patients initially sought care in private facilities, which had considerably less tuberculosis diagnostic capacity than public facilities; only 7% of notified cases were from the private sector. The GeneXpert system was available in 14%-41% of level 2 facilities in the 3 countries for which there were data. Tuberculosis treatment capacity tracked closely with the availability of diagnostic capacity. There were substantial subnational differences in care-seeking patterns and service availability.
Discussion: The PPA can be a valuable planning and programming tool to ensure that diagnostic and treatment services are available to patients where they seek care. Patient-centered care will require closing the diagnostic gap and engaging the private sector. Extensive subnational differences in patient pathways to care call for differentiated approaches to patient-centered care.
Keywords: Tuberculosis; care seeking; patient-pathway analysis; private sector.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures


References
-
- United Nations Millennium Project. Goals, targets, and indicators 2000. http://www.unmillenniumproject.org/goals/gti.htm. Accessed 2 June 2017.
-
- World Health Organization. Global tuberculosis Report 2016. http://www.who.int/tb/publications/global_report/en/. Accessed 2 June 2017.
-
- World Health Organization. Global Health Observatory (GHO) data for tuberculosis 2015. http://www.who.int/gho/tb/en/. Accessed 2 June 2017.
-
- United Nations. Sustainable Development Goals: Goal 3 2015. http://www.un.org/sustainabledevelopment/health/. Accessed 2 June 2017.
-
- World Health Organization. The top 10 causes of death 2015. http://www.who.int/mediacentre/factsheets/fs310/en/. Accessed 2 June 2017.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
