

Using Patient Pathway Analysis to Design Patient-centered Referral Networks for Diagnosis and Treatment of Tuberculosis: The Case of the Philippines
- PMID: 29117352
- PMCID: PMC5853338
- DOI: 10.1093/infdis/jix391
Using Patient Pathway Analysis to Design Patient-centered Referral Networks for Diagnosis and Treatment of Tuberculosis: The Case of the Philippines
Abstract
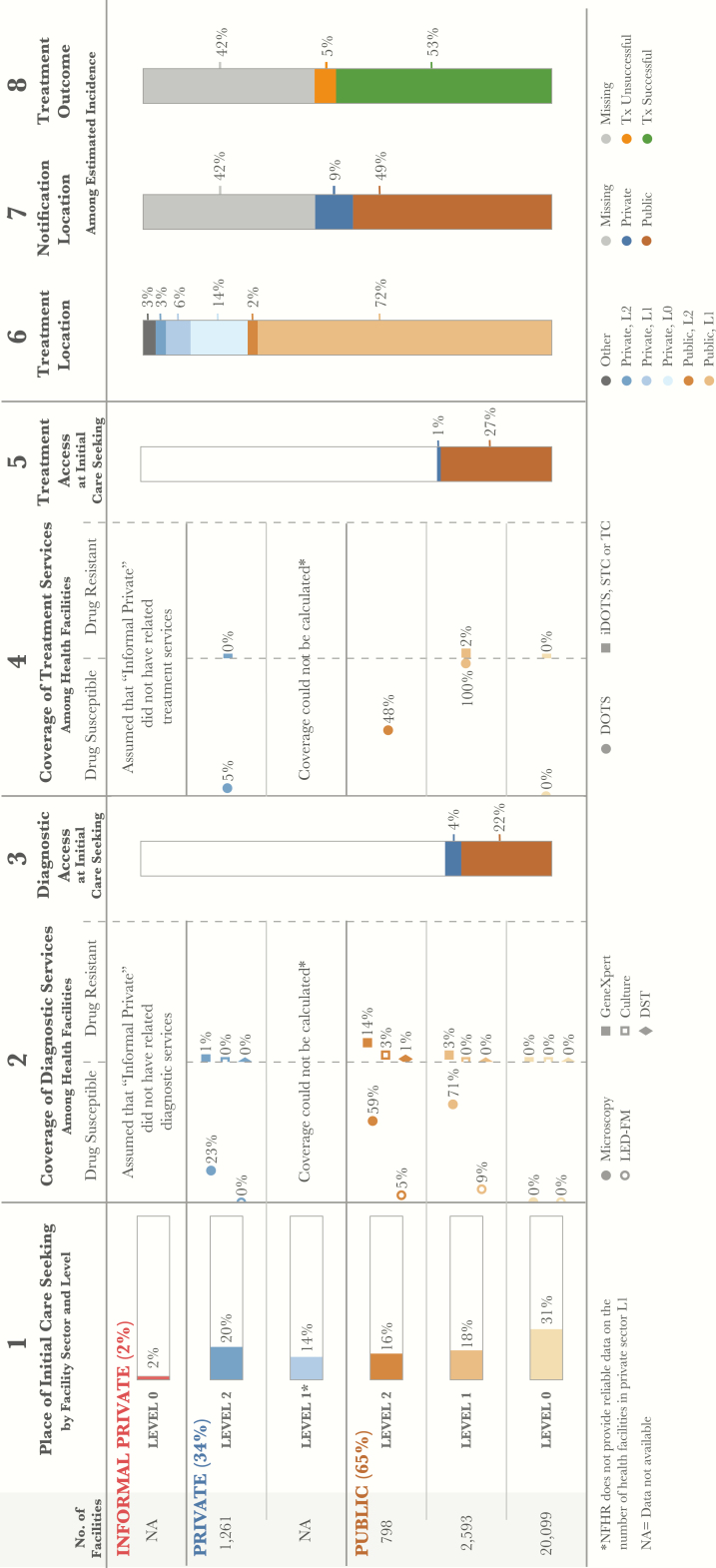
Background: Tuberculosis (TB) is the 8th leading cause of death in the Philippines. A recent prevalence survey found that there were nearly 70% more cases of tuberculosis than previously estimated. Given these new data, the National TB Program (NTP), operating through a decentralized health system, identified about 58% of the estimated new drug-sensitive (DS) TB patients in 2016. However, the NTP only identified and commenced treatment for around 17% of estimated new drug-resistant patients. In order to reach the remaining 42% of drug-sensitive patients and 83% of drug-resistant patients, it is necessary to develop a better understanding of where patients seek care.
Methods: National and regional patient pathway analyses (PPAs) were undertaken using existing national survey and NTP data. The PPA assessed the alignment between patient care seeking and the availability of TB diagnostic and treatment services.
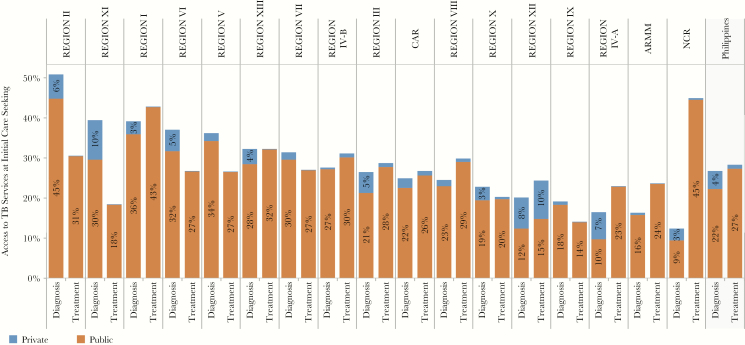
Results: Systemic referral networks from the community-level Barangay Health Stations (BHSs) to diagnostic facilities have enabled more efficient detection of drug-sensitive tuberculosis in the public sector. Approximately 36% of patients initiated care in the private sector, where there is limited coverage of appropriate diagnostic technologies. Important differences in the alignment between care seeking patterns and diagnostic and treatment availability were found between regions.
Conclusions: The PPA identified opportunities for strengthening access to care for all forms of tuberculosis and for accelerating the time to diagnosis by aligning services to where patients initiate care. Geographic variations in care seeking may guide prioritization of some regions for intensified engagement with the private sector.
Keywords: MDR-TB; care seeking; diagnosis; patient pathway analysis; tuberculosis.
© The Author 2017. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- United Nations General Assembly. Transforming our World: The 2030 Agenda for Sustainable Development, 2015 Available at: https://www.un.org/pga/wpcontent/uploads/sites/3/2015/08/120815_outcome-.... Accessed 1 May 2017.
-
- Philippines Statistics Authority. Census of Population, 2015 Available at https://psa.gov.ph/statistics/census/population-and-housing. Accessed 1 May 2017.
-
- United Nations Department of Economic and Social Affairs. Sustainability Development Knowledge Platform Available at: https://sustainabledevelopment.un.org/hlpf/2016/philippines. Accessed 1 May 2017.
-
- Philippines National Tuberculosis Program. Joint Tuberculosis Program Review, 2016 Available at: http://www.ntp.doh.gov.ph/downloads/publications/JPR_2016_ecopy.pdf. Accessed 1 May 2017.
-
- Philippines Department of Health. National Objectives for Health 2011–2016 Available At: http://www.doh.gov.ph/sites/default/files/publications/noh2016.pdf. Accessed 1 May 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
