

Induced Pluripotent Stem Cell (iPSC)-Derived Extracellular Vesicles Are Safer and More Effective for Cardiac Repair Than iPSCs
- PMID: 29118058
- PMCID: PMC5775034
- DOI: 10.1161/CIRCRESAHA.117.311769
Induced Pluripotent Stem Cell (iPSC)-Derived Extracellular Vesicles Are Safer and More Effective for Cardiac Repair Than iPSCs
Abstract
Rationale: Extracellular vesicles (EVs) are tiny membrane-enclosed droplets released by cells through membrane budding or exocytosis. The myocardial reparative abilities of EVs derived from induced pluripotent stem cells (iPSCs) have not been directly compared with the source iPSCs.
Objective: To examine whether iPSC-derived EVs can influence the biological functions of cardiac cells in vitro and to compare the safety and efficacy of iPSC-derived EVs (iPSC-EVs) and iPSCs for cardiac repair in vivo.
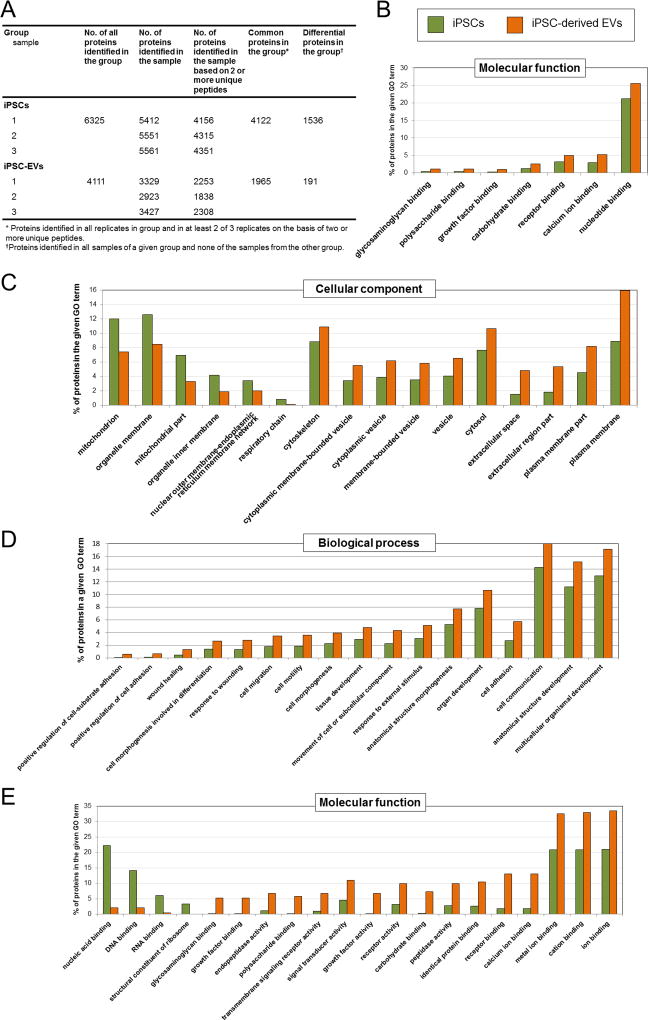
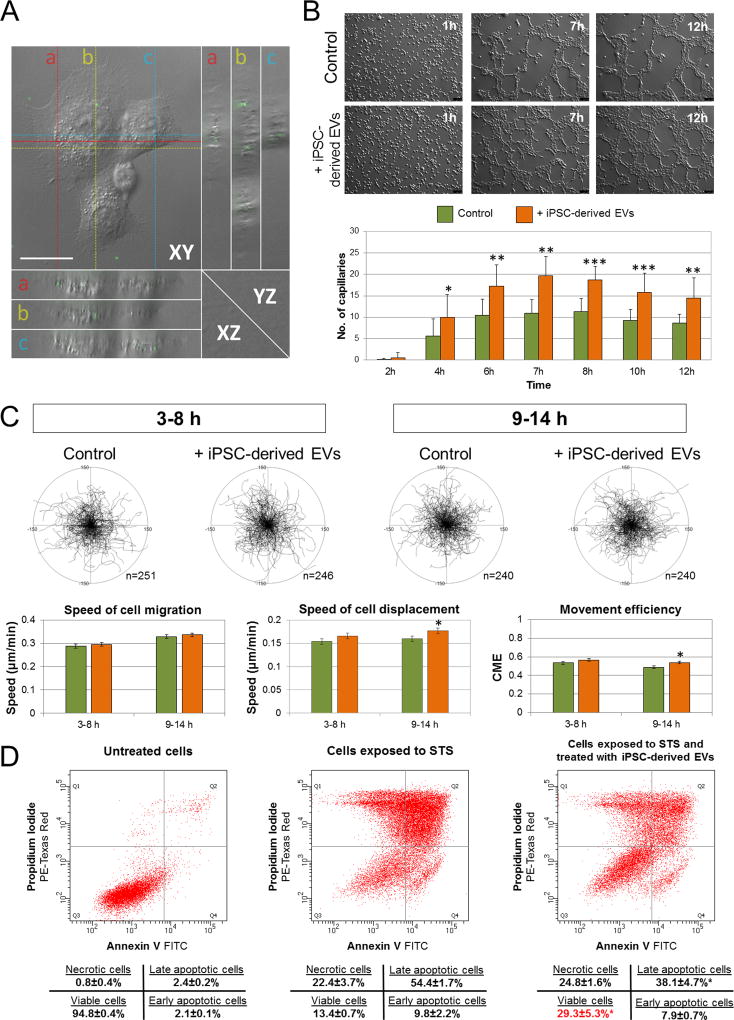
Methods and results: Murine iPSCs were generated, and EVs isolated from culture supernatants by sequential centrifugation. Atomic force microscopy, high-resolution flow cytometry, real-time quantitative RT-PCR, and mass spectrometry were used to characterize EV morphology and contents. iPSC-EVs were enriched in miRNAs and proteins with proangiogenic and cytoprotective properties. iPSC-EVs enhanced angiogenic, migratory, and antiapoptotic properties of murine cardiac endothelial cells in vitro. To compare the cardiac reparative capacities in vivo, vehicle, iPSCs, and iPSC-EVs were injected intramyocardially at 48 hours after a reperfused myocardial infarction in mice. Compared with vehicle-injected mice, both iPSC- and iPSC-EV-treated mice exhibited improved left ventricular function at 35 d after myocardial infarction, albeit iPSC-EVs rendered greater improvement. iPSC-EV injection also resulted in reduction in left ventricular mass and superior perfusion in the infarct zone. Both iPSCs and iPSC-EVs preserved viable myocardium in the infarct zone, whereas reduction in apoptosis was significant with iPSC-EVs. iPSC injection resulted in teratoma formation, whereas iPSC-EV injection was safe.
Conclusions: iPSC-derived EVs impart cytoprotective properties to cardiac cells in vitro and induce superior cardiac repair in vivo with regard to left ventricular function, vascularization, and amelioration of apoptosis and hypertrophy. Because of their acellular nature, iPSC-EVs represent a safer alternative for potential therapeutic applications in patients with ischemic myocardial damage.
Keywords: angiogenesis; apoptosis; extracellular vesicles; induced pluripotent stem cells; myocardial infarction; remodeling; stem cells.
© 2017 American Heart Association, Inc.
Figures






Comment in
-
Induced Pluripotent Stem Cells Derived Extracellular Vesicles: A Potential Therapy for Cardiac Repair.Circ Res. 2018 Jan 19;122(2):197-198. doi: 10.1161/CIRCRESAHA.117.312394. Circ Res. 2018. PMID: 29348245 Free PMC article. No abstract available.
References
-
- Bobis-Wozowicz S, Kmiotek K, Sekula M, Kedracka-Krok S, Kamycka E, Adamiak M, Jankowska U, Madetko-Talowska A, Sarna M, Bik-Multanowski M, Kolcz J, Boruczkowski D, Madeja Z, Dawn B, Zuba-Surma EK. Human Induced Pluripotent Stem Cell-Derived Microvesicles Transmit RNAs and Proteins to Recipient Mature Heart Cells Modulating Cell Fate and Behavior. Stem Cells. 2015;33:2748–2761. - PubMed
-
- Thery C, Zitvogel L, Amigorena S. Exosomes: composition, biogenesis and function. Nat Rev Immunol. 2002;2:569–579. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
