

Complement Activation via a C3a Receptor Pathway Alters CD4+ T Lymphocytes and Mediates Lung Cancer Progression
- PMID: 29118090
- PMCID: PMC5810934
- DOI: 10.1158/0008-5472.CAN-17-0240
Complement Activation via a C3a Receptor Pathway Alters CD4+ T Lymphocytes and Mediates Lung Cancer Progression
Abstract
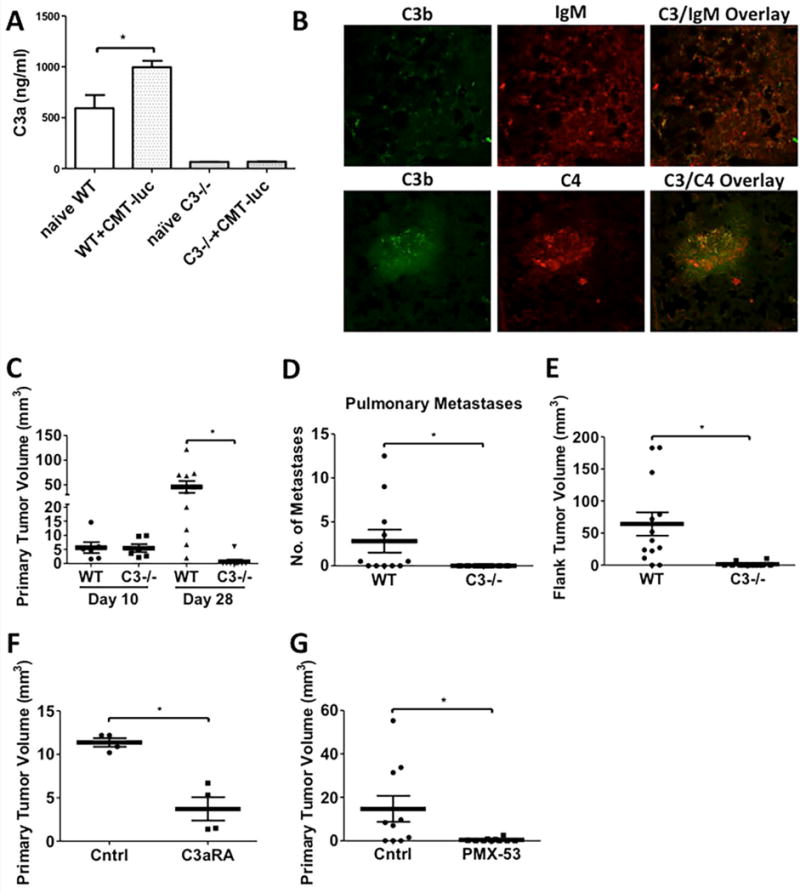
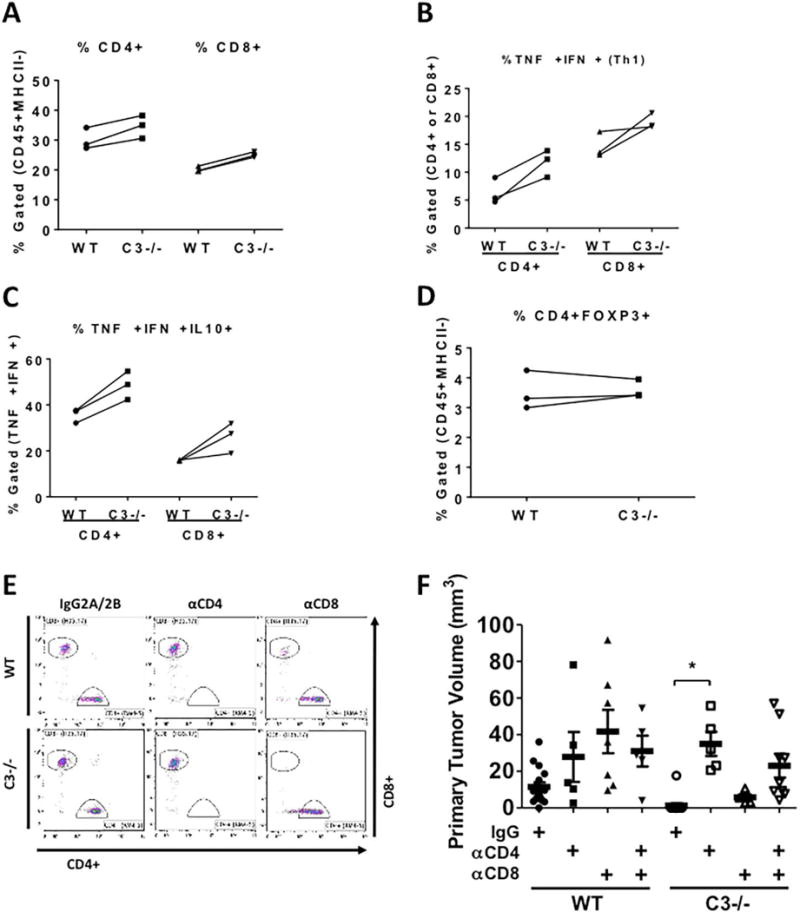
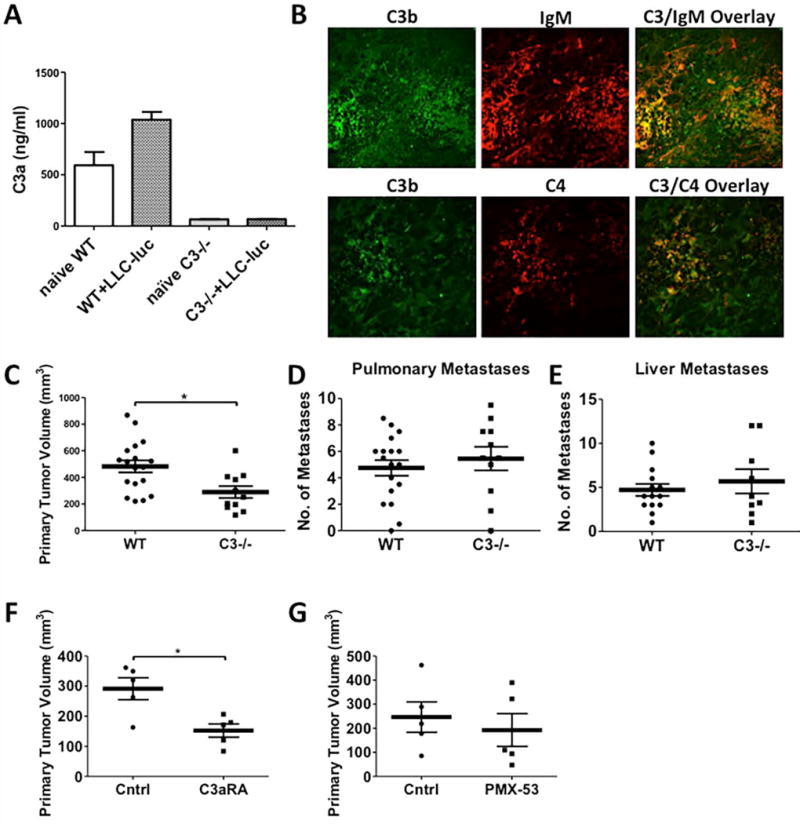
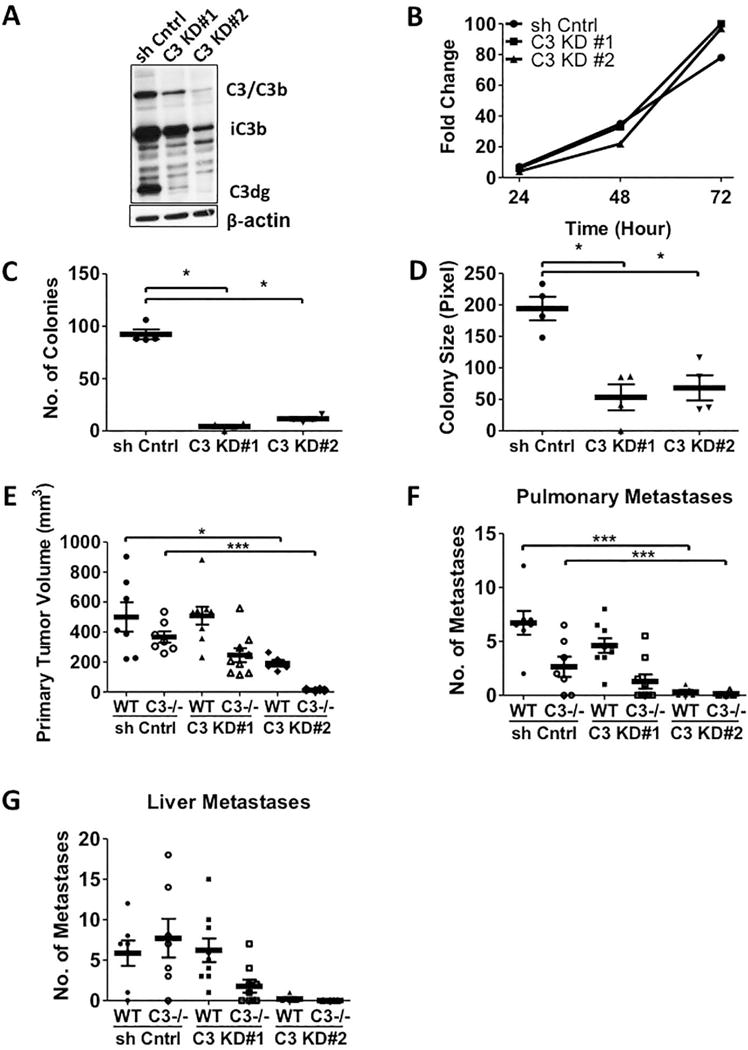
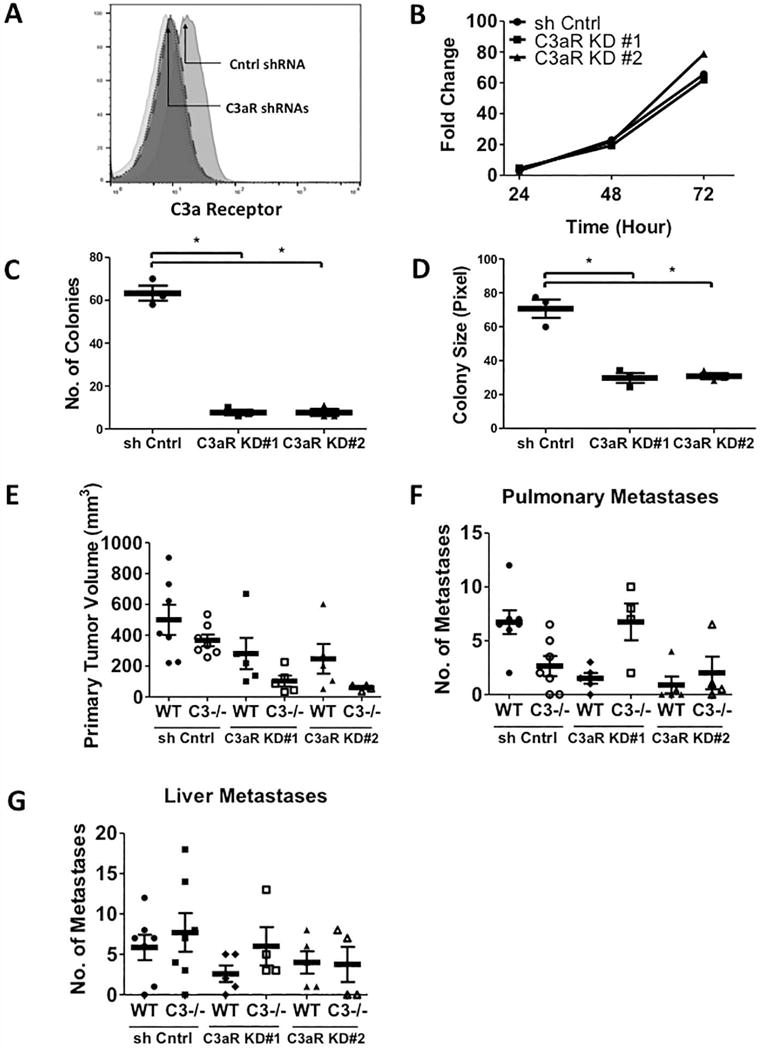
The complement cascade is a part of the innate immune system that acts primarily to remove pathogens and injured cells. However, complement activation is also peculiarly associated with tumor progression. Here we report mechanistic insights into this association in multiple immunocompetent orthotopic models of lung cancer. After tumor engraftment, we observed systemic activation of the complement cascade as reflected by elevated levels of the key regulator C3a. Notably, growth of primary tumors and metastases was both strongly inhibited in C3-deficient mice (C3-/- mice), with tumors undetectable in many subjects. Growth inhibition was associated with increased numbers of IFNγ+/TNFα+/IL10+ CD4+ and CD8+ T cells. Immunodepletion of CD4+ but not CD8+ T cells in tumor-bearing subjects reversed the inhibitory effects of C3 deletion. Similarly, antagonists of the C3a or C5a receptors inhibited tumor growth. Investigations using multiple tumor cell lines in the orthotopic model suggested the involvement of a C3/C3 receptor autocrine signaling loop in regulating tumor growth. Overall, our findings offer functional evidence that complement activation serves as a critical immunomodulator in lung cancer progression, acting to drive immune escape via a C3/C5-dependent pathway.Significance: This provocative study suggests that inhibiting complement activation may heighten immunotherapeutic responses in lung cancer, offering findings with immediate implications, given the existing clinical availability of complement antagonists. Cancer Res; 78(1); 143-56. ©2017 AACR.
©2017 American Association for Cancer Research.
Figures
Comment in
-
How complement activation via a C3a receptor pathway alters CD4+ T lymphocytes and mediates lung cancer progression?-future perspectives.J Thorac Dis. 2019 Mar;11(Suppl 3):S210-S211. doi: 10.21037/jtd.2019.02.21. J Thorac Dis. 2019. PMID: 30997178 Free PMC article. No abstract available.
References
-
- Hollenberg NK. Hypertension and the kidney: determinants of the response to antihypertensive therapy and their implications. Am Heart J. 1993;125:604–8. - PubMed
-
- Gettinger SN, Horn L, Gandhi L, Spigel DR, Antonia SJ, Rizvi NA, Powderly JD, Heist RS, Carvajal RD, Jackman DM, Sequist LV, Smith DC, Leming P, Carbone DP, Pinder-Schenck MC, Topalian SL, Hodi FS, Sosman JA, Sznol M, McDermott DF, Pardoll DM, Sankar V, Ahlers CM, Salvati M, Wigginton JM, Hellmann MD, Kollia GD, Gupta AK, Brahmer JR. Overall Survival and Long-Term Safety of Nivolumab (Anti-Programmed Death 1 Antibody, BMS-936558, ONO-4538) in Patients With Previously Treated Advanced Non-Small-Cell Lung Cancer. J Clin Oncol. 2015;33:2004–12. - PMC - PubMed
-
- Oner F, Savas I, Numanoglu N. Immunoglobulins and complement components in patients with lung cancer. Tuberk Toraks. 2004;52:19–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
