

Preventing progression from arthralgia to arthritis: targeting the right patients
- PMID: 29118439
- PMCID: PMC6298577
- DOI: 10.1038/nrrheum.2017.185
Preventing progression from arthralgia to arthritis: targeting the right patients
Abstract
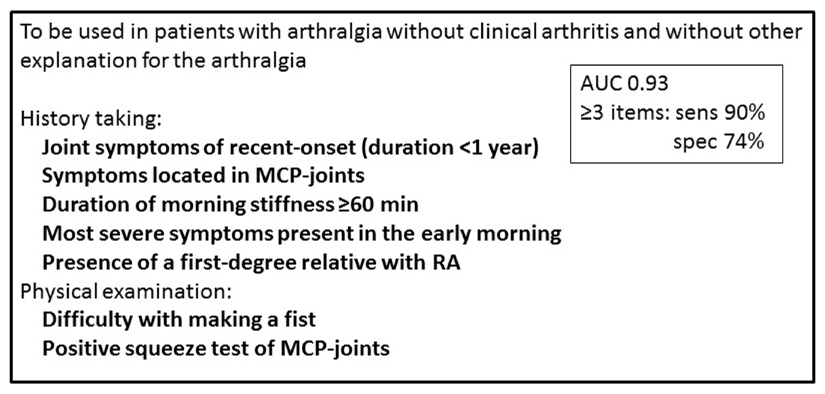
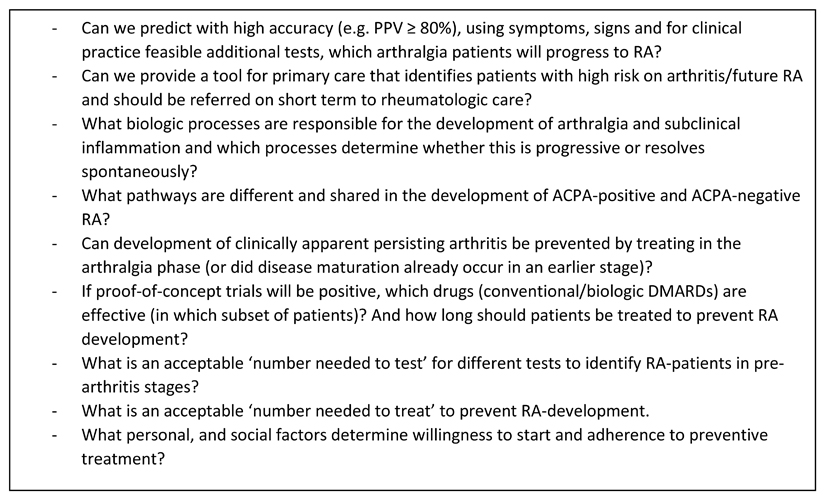
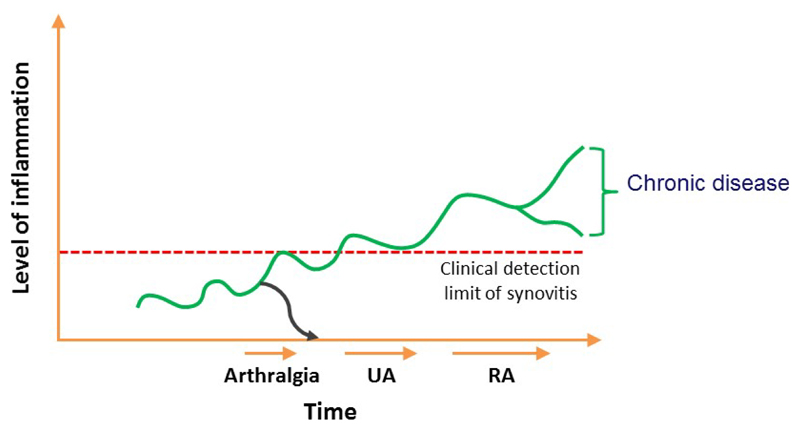
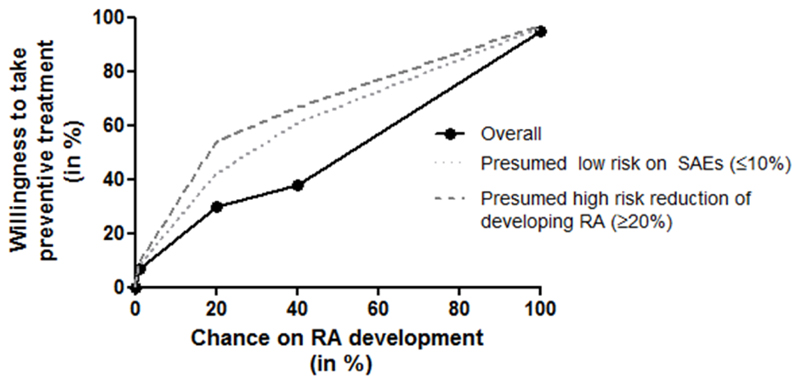
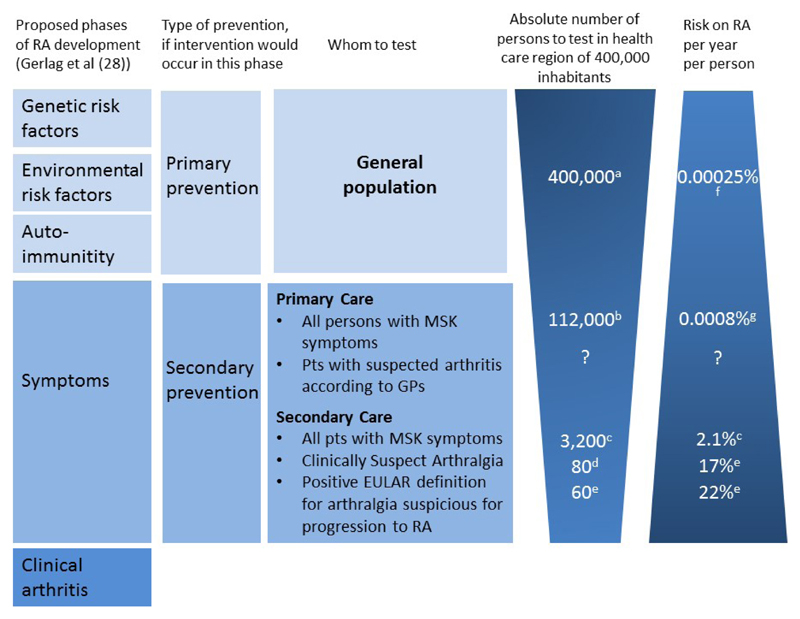
Early treatment is associated with improved outcomes in patients with rheumatoid arthritis (RA), suggesting that a 'window of opportunity', in which the disease is most susceptible to disease-modifying treatment, exists. Autoantibodies and markers of systemic inflammation can be present long before clinical arthritis, and maturation of the immune response seems to coincide with the development of RA. The pre-arthritis phase associated with symptoms such as as joint pain without clinical arthritis (athralgia) is now hypothesized to fall within the aforementioned window of opportunity. Consequently, disease modulation in this phase might prevent the occurrence of clinically apparent arthritis, which would result in a persistent disease course if untreated. Several ongoing proof-of-concept trials are now testing this hypothesis. This Review highlights the importance of adequate risk prediction for the correct design, execution and interpretation of results of these prevention trials, as well as considerations when translating these findings into clinical practice. The patients' perspectives are discussed, and the accuracy with which RA development can be predicted in patients presenting with arthralgia is evaluated. Currently, the best starting position for preventive studies is proposed to be the inclusion of patients with an increased risk of RA, such as those identified as fulfilling the EULAR definition of 'arthralgia suspicious for progression to RA'.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Combe B, Landewe R, Daien CI, Hua C, Aletaha D, Álvaro-Gracia JM, et al. 2016 update of the EULAR recommendations for the management of early arthritis. Ann Rheum Dis. 2017 Jun 1;76(6):948–959. - PubMed
-
- Boers M. Understanding the window of opportunity concept in early rheumatoid arthritis. Arthritis Rheum. 2003 Jul 1;48(7):1771–4. - PubMed
-
- van Nies JA, Tsonaka R, Gaujoux-Viala C, Fautrel B, van der Helm-van Mil AHM. Evaluating relationships between symptom duration and persistence of rheumatoid arthritis: does a window of opportunity exist? Results on the Leiden Early Arthritis Clinic and ESPOIR cohorts. Ann Rheum Dis. 2015 May 1;74(5):806–12. - PubMed
-
- Ajeganova S, van Steenbergen HW, van Nies JAB, Burgers LE, Huizinga TWJ, van der Helm-van Mil AHM. Disease-modifying antirheumatic drug-free sustained remission in rheumatoid arthritis: an increasingly achievable outcome with subsidence of disease symptoms. Ann Rheum Dis. 2016 May 1;75(5):867–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
