

Metastatic breast cancer: Endocrine therapy landscape reshaped
- PMID: 29119080
- PMCID: PMC5655644
- DOI: 10.4103/ajm.AJM_20_17
Metastatic breast cancer: Endocrine therapy landscape reshaped
Abstract
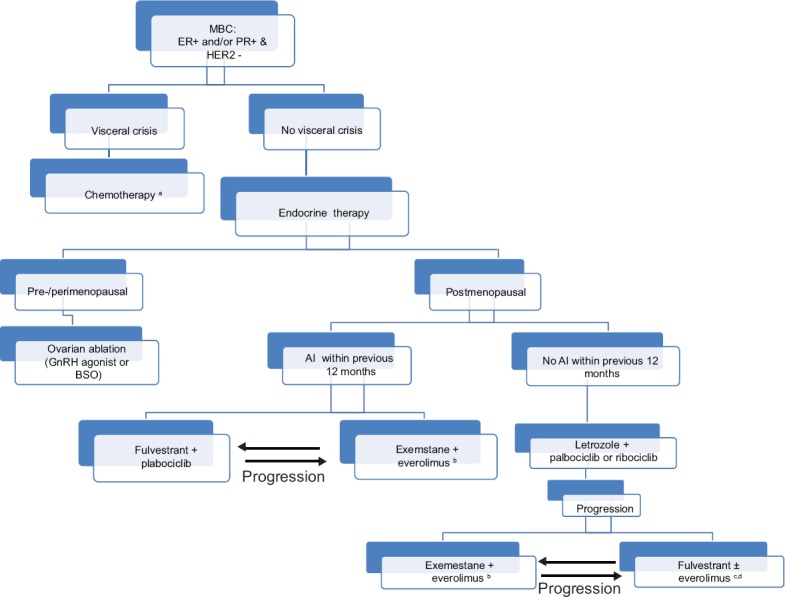
Endocrine therapy (ET) of hormone receptor (HR)-positive and human epidermal growth factor receptor 2-(HER2)-negative metastatic breast cancer (MBC) historically focused on estrogen deprivation and antagonism. The identification of several intracellular pathways promoting resistance to antiestrogen therapy led to the introduction of novel endocrine drug combinations that reformed treatment schema and expanded therapeutic options. There is no doubt that efforts to overcome or delay resistance to ET are fruiting, particularly with the introduction of cyclin-dependent kinase 4/6 inhibitors such as palbociclib and ribociclib, and mechanistic target of rapamycin inhibitors such as everolimus. Although still considered incurable by currently available treatment modalities, many patients with MBC nowadays enjoy several years of good quality life coupled with decent tumor control. The diversity of therapies and unusual pattern of side effects can be quite perplexing to the treating physician. The sequence of variable agents and management of side effects, in addition to the timing of initiation of cytotoxic chemotherapy, is among the challenges faced by oncologists. In this review, we shed a spotlight on mechanisms of resistance to ET, and provide a review of landmark studies that have recently reshaped the landscape of treatment options for patients with metastatic HR-positive, HER2-negative MBC. A suggested treatment strategy for newly diagnosed patients is also discussed herein.
Keywords: Breast cancer; endocrine therapy; metastatic.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Based on November 2015 SEER Data Submission, Posted April, 2016. Bethesda, MD: National Cancer Institute; [Last accessed on 2016 Dec 01]. SEER Cancer Statistics Review, 1975-2013. Available from: http://www.seer.cancer.gov/csr/1975_2013/
-
- van de Water W, Markopoulos C, van de Velde CJ, Seynaeve C, Hasenburg A, Rea D, et al. Association between age at diagnosis and disease-specific mortality among postmenopausal women with hormone receptor-positive breast cancer. JAMA. 2012;307:590–7. - PubMed
-
- O'Shaughnessy J. Extending survival with chemotherapy in metastatic breast cancer. Oncologist. 2005;10(Suppl 3):20–9. - PubMed
-
- Zeichner SB, Herna S, Mani A, Ambros T, Montero AJ, Mahtani RL, et al. Survival of patients with de-novo metastatic breast cancer: Analysis of data from a large breast cancer-specific private practice, a university-based cancer center and review of the literature. Breast Cancer Res Treat. 2015;153:617–24. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous