

Surveillance for Lyme Disease - United States, 2008-2015
- PMID: 29120995
- PMCID: PMC5829628
- DOI: 10.15585/mmwr.ss6622a1
Surveillance for Lyme Disease - United States, 2008-2015
Abstract
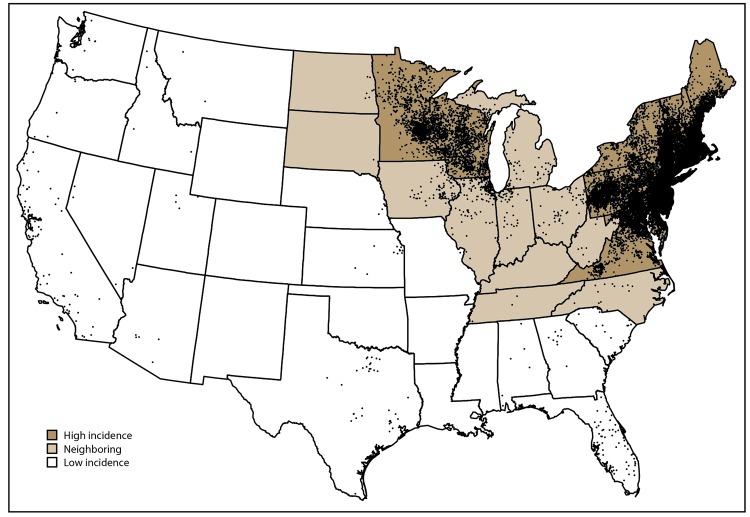
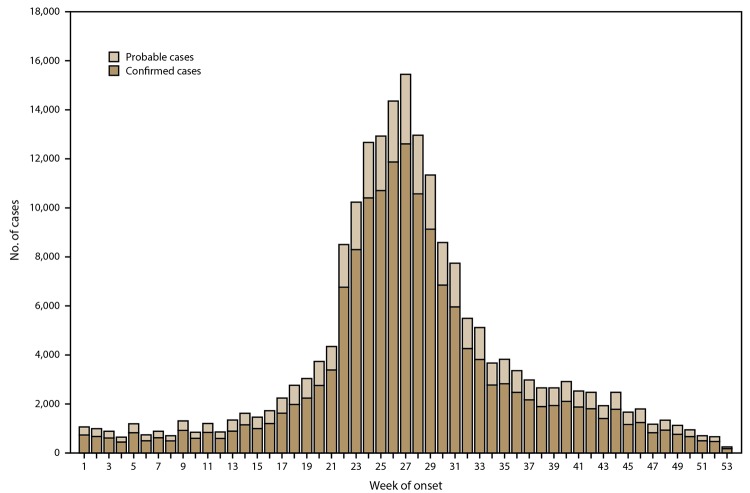
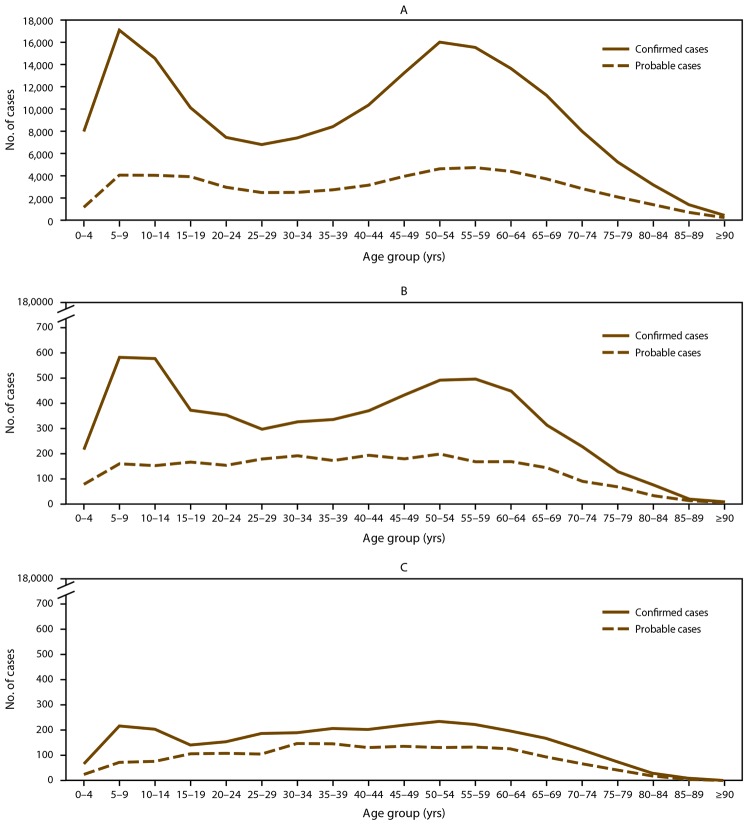
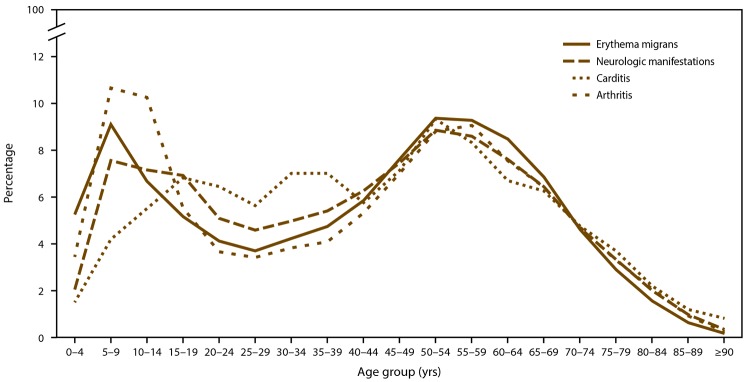
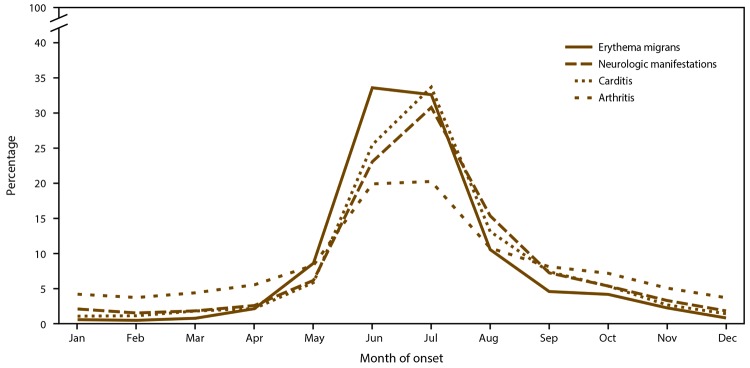
Problem/condition: Lyme disease is the most commonly reported vectorborne disease in the United States but is geographically focal. The majority of Lyme disease cases occur in the Northeast, mid-Atlantic, and upper Midwest regions. Lyme disease can cause varied clinical manifestations, including erythema migrans, arthritis, facial palsy, and carditis. Lyme disease occurs most commonly among children and older adults, with a slight predominance among males.
Reporting period: 2008-2015.
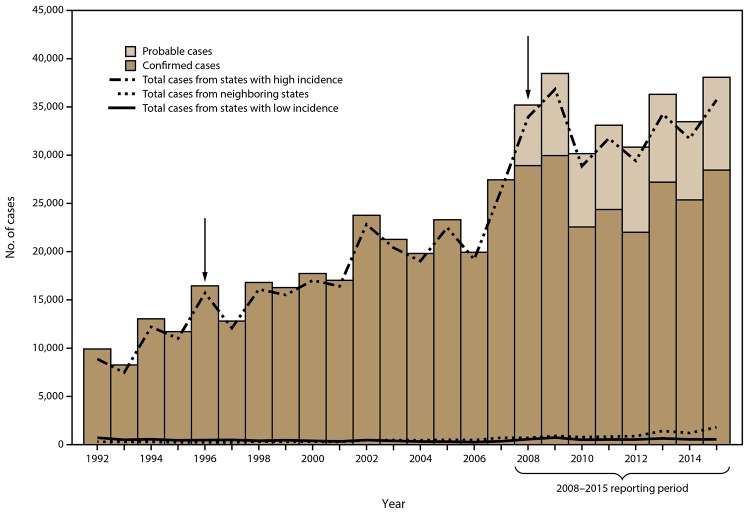
Description of system: Lyme disease has been a nationally notifiable condition in the United States since 1991. Possible Lyme disease cases are reported to local and state health departments by clinicians and laboratories. Health department staff conduct case investigations to classify cases according to the national surveillance case definition. Those that qualify as confirmed or probable cases of Lyme disease are reported to CDC through the National Notifiable Diseases Surveillance System. States with an average annual incidence during this reporting period of ≥10 confirmed Lyme disease cases per 100,000 population were classified as high incidence. States that share a border with those states or that are located between areas of high incidence were classified as neighboring states. All other states were classified as low incidence.
Results: During 2008-2015, a total of 275,589 cases of Lyme disease were reported to CDC (208,834 confirmed and 66,755 probable). Although most cases continue to be reported from states with high incidence in the Northeast, mid-Atlantic, and upper Midwest regions, case counts in most of these states have remained stable or decreased during the reporting period. In contrast, case counts have increased in states that neighbor those with high incidence. Overall, demographic characteristics associated with confirmed cases were similar to those described previously, with a slight predominance among males and a bimodal age distribution with peaks among young children and older adults. Yet, among the subset of cases reported from states with low incidence, infection occurred more commonly among females and older adults. In addition, probable cases occurred more commonly among females and with a higher modal age than confirmed cases.
Interpretation: Lyme disease continues to be the most commonly reported vectorborne disease in the United States. Although concentrated in historically high-incidence areas, the geographic distribution is expanding into neighboring states. The trend of stable to decreasing case counts in many states with high incidence could be a result of multiple factors, including actual stabilization of disease incidence or artifact due to modifications in reporting practices employed by some states to curtail the resource burden associated with Lyme disease surveillance.
Public health action: This report highlights the continuing public health challenge of Lyme disease in states with high incidence and demonstrates its emergence in neighboring states that previously experienced few cases. Educational efforts should be directed accordingly to facilitate prevention, early diagnosis, and appropriate treatment. As Lyme disease emerges in neighboring states, clinical suspicion of Lyme disease in a patient should be based on local experience rather than incidence cutoffs used for surveillance purposes. A diagnosis of Lyme disease should be considered in patients with compatible clinical signs and a history of potential exposure to infected ticks, not only in states with high incidence but also in areas where Lyme disease is known to be emerging. These findings underscore the ongoing need to implement personal prevention practices routinely (e.g., application of insect repellent and inspection for and removal of ticks) and to develop other effective interventions.
Figures
References
-
- Steere AC. Lyme disease (Lyme borreliosis) due to Borrelia burgdorferi [Chapter 242]. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases. 8th ed. Philadelphia, PA: Elsevier/Saunders; 2015:2725–35.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical