

Unchanging premature mortality trends in systemic lupus erythematosus: a general population-based study (1999-2014)
- PMID: 29121273
- PMCID: PMC5850281
- DOI: 10.1093/rheumatology/kex412
Unchanging premature mortality trends in systemic lupus erythematosus: a general population-based study (1999-2014)
Abstract
Objective: Patients with SLE have increased morbidity and premature mortality. Whether this mortality gap has improved in recent years, as in RA, is unknown.
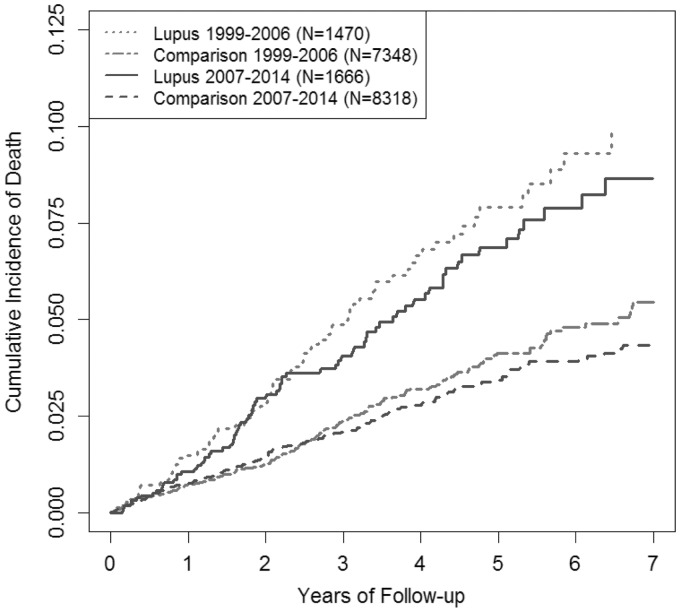
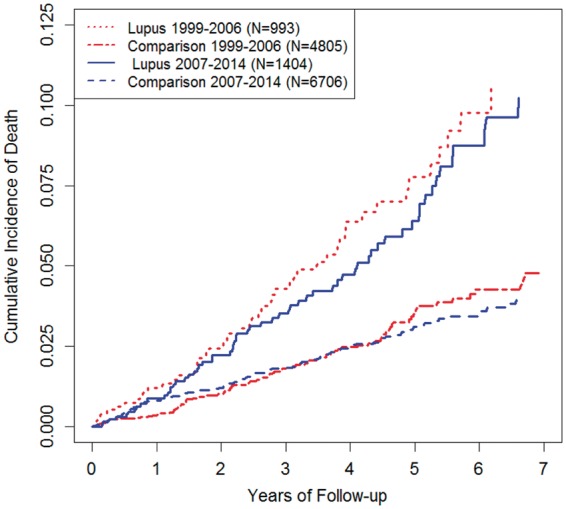
Methods: We conducted a population-based cohort study using a medical records database representative of the general population of the UK. We identified incident SLE cases and matched non-SLE controls between 1999 and 2014, divided into two subgroups based on year of SLE diagnosis, forming the early cohort (1999-2006) and late cohort (2007-14). We compared the mortality rates and hazard ratios, adjusting for potential confounders.
Results: We identified 1470 and 1666 incident SLE cases in the early and late cohorts, respectively. In both cohorts, SLE patients had similar levels of excess mortality compared with their matched comparators [15.9 vs 7.9 deaths/1000 person-years (PY) in the early cohort and 13.8 vs 7.0 deaths/1000 PY in the late cohort]. The corresponding mortality hazard ratios were 2.15 (95% CI 1.63, 2.83) and 2.12 (95% CI 1.61, 2.80) in the early and late cohorts, respectively (P-value for interaction = 0.95). The absolute mortality differences were 8.0 (95% CI 4.3, 11.8) and 6.8 (95% CI 3.5, 10.0) deaths/1000 PY, respectively (P-value for interaction = 0.61).
Conclusion: This general population-based cohort study suggests that excess mortality has not improved among SLE patients in recent years, remaining greater than double that of comparators, unlike RA during the same period. This highlights a critical unmet need for the development of new therapeutic agents and improved management strategies for SLE and its comorbidities.
Keywords: lupus; mortality; quality of care; treatment; trend analysis.
© The Author 2017. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For Permissions, please email: journals.permissions@oup.com
Figures
References
-
- Abu-Shakra M, Gladman DD, Urowitz MB.. Mortality studies in SLE: how far can we improve survival of patients with SLE. Autoimmun Rev 2004;3:418–20. - PubMed
-
- Borchers AT, Keen CL, Shoenfeld Y, Gershwin ME.. Surviving the butterfly and the wolf: mortality trends in systemic lupus erythematosus. Autoimmun Rev 2004;3:423–53. - PubMed
-
- Lee Y, Choi S, Ji J, Song G.. Overall and cause-specific mortality in systemic lupus erythematosus: an updated meta-analysis. Lupus 2016;25:727–34. - PubMed
-
- Urowitz M, Bookman A, Koehler B. et al. The bimodal mortality pattern of systemic lupus erythematosus. Am J Med 1976;60:221–5. - PubMed
-
- Aviña-Zubieta JA. Risk of myocardial infarction and stroke in newly diagnosed systemic lupus erythematosus: a general population-based study. Arthritis Care Res 2017;69:849–56. [WorldCat] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
