

Placental Drug Transport-on-a-Chip: A Microengineered In Vitro Model of Transporter-Mediated Drug Efflux in the Human Placental Barrier
- PMID: 29121458
- PMCID: PMC5793852
- DOI: 10.1002/adhm.201700786
Placental Drug Transport-on-a-Chip: A Microengineered In Vitro Model of Transporter-Mediated Drug Efflux in the Human Placental Barrier
Abstract
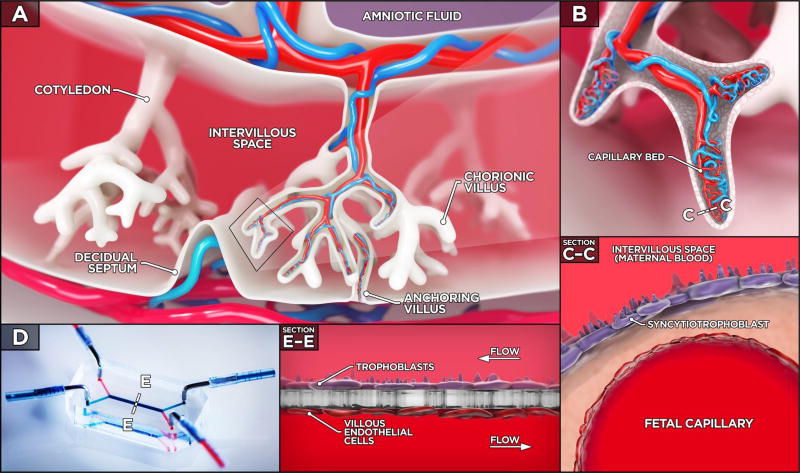
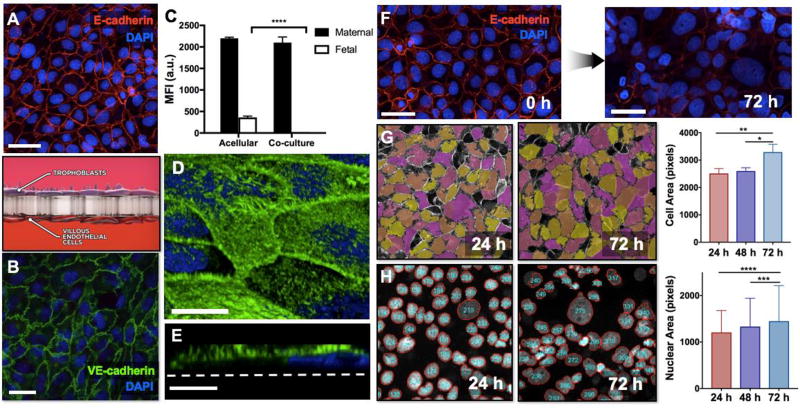
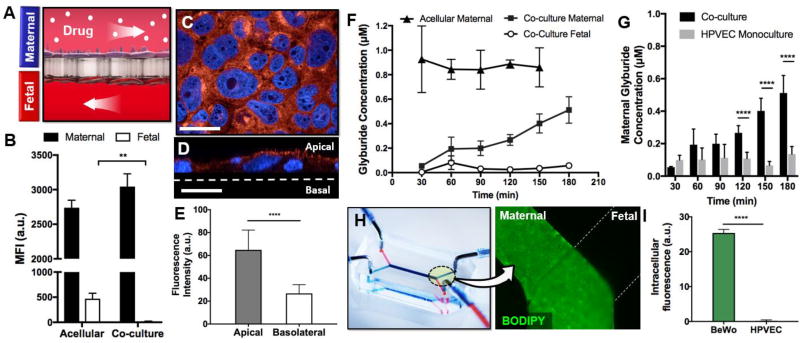
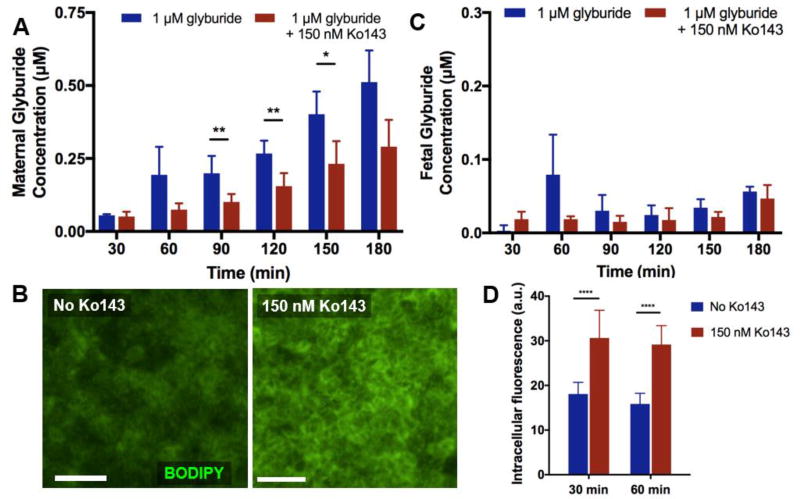
The current lack of knowledge about the effect of maternally administered drugs on the developing fetus is a major public health concern worldwide. The first critical step toward predicting the safety of medications in pregnancy is to screen drug compounds for their ability to cross the placenta. However, this type of preclinical study has been hampered by the limited capacity of existing in vitro and ex vivo models to mimic physiological drug transport across the maternal-fetal interface in the human placenta. Here the proof-of-principle for utilizing a microengineered model of the human placental barrier to simulate and investigate drug transfer from the maternal to the fetal circulation is demonstrated. Using the gestational diabetes drug glyburide as a model compound, it is shown that the microphysiological system is capable of reconstituting efflux transporter-mediated active transport function of the human placental barrier to limit fetal exposure to maternally administered drugs. The data provide evidence that the placenta-on-a-chip may serve as a new screening platform to enable more accurate prediction of drug transport in the human placenta.
Keywords: drug transport; glyburide; placenta-on-a-chip.
© 2017 WILEY-VCH Verlag GmbH & Co. KGaA, Weinheim.
Figures
Similar articles
-
A microphysiological model of the human placental barrier.Lab Chip. 2016 Aug 2;16(16):3065-73. doi: 10.1039/c6lc00259e. Lab Chip. 2016. PMID: 27229450 Free PMC article.
-
Placenta-on-a-chip: a novel platform to study the biology of the human placenta.J Matern Fetal Neonatal Med. 2016;29(7):1046-54. doi: 10.3109/14767058.2015.1038518. Epub 2015 Jun 15. J Matern Fetal Neonatal Med. 2016. PMID: 26075842 Free PMC article.
-
Evaluation of a microphysiological human placental barrier model for studying placental drug transfer.Reprod Toxicol. 2024 Jan;123:108523. doi: 10.1016/j.reprotox.2023.108523. Epub 2023 Dec 12. Reprod Toxicol. 2024. PMID: 38092131
-
Placenta-on-a-Chip as an In Vitro Approach to Evaluate the Physiological and Structural Characteristics of the Human Placental Barrier upon Drug Exposure: A Systematic Review.J Clin Med. 2023 Jun 27;12(13):4315. doi: 10.3390/jcm12134315. J Clin Med. 2023. PMID: 37445348 Free PMC article. Review.
-
Placental microphysiological systems: new advances on promising platforms that mimic the microenvironment of the human placenta.Lab Chip. 2025 Feb 25;25(5):979-995. doi: 10.1039/d4lc00500g. Lab Chip. 2025. PMID: 39417748 Review.
Cited by
-
Fabrication of Concave Microwells and Their Applications in Micro-Tissue Engineering: A Review.Micromachines (Basel). 2022 Sep 19;13(9):1555. doi: 10.3390/mi13091555. Micromachines (Basel). 2022. PMID: 36144178 Free PMC article. Review.
-
Organ-on-a-chip for perinatal biology experiments.Placenta Reprod Med. 2022 Jul 6;1:98. Epub 2022 Aug 29. Placenta Reprod Med. 2022. PMID: 36530581 Free PMC article.
-
Optimization of the TeraTox Assay for Preclinical Teratogenicity Assessment.Toxicol Sci. 2022 Jun 28;188(1):17-33. doi: 10.1093/toxsci/kfac046. Toxicol Sci. 2022. PMID: 35485993 Free PMC article.
-
Placenta Disrupted: Endocrine Disrupting Chemicals and Pregnancy.Trends Endocrinol Metab. 2020 Jul;31(7):508-524. doi: 10.1016/j.tem.2020.03.003. Epub 2020 Apr 2. Trends Endocrinol Metab. 2020. PMID: 32249015 Free PMC article. Review.
-
The Application of Engineered Nanomaterials in Perinatal Therapeutics.Small. 2024 Oct;20(41):e2303072. doi: 10.1002/smll.202303072. Epub 2023 Jul 12. Small. 2024. PMID: 37438678 Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
