

Palliative Care Planner: A Pilot Study to Evaluate Acceptability and Usability of an Electronic Health Records System-integrated, Needs-targeted App Platform
- PMID: 29121480
- PMCID: PMC5812235
- DOI: 10.1513/AnnalsATS.201706-500OC
Palliative Care Planner: A Pilot Study to Evaluate Acceptability and Usability of an Electronic Health Records System-integrated, Needs-targeted App Platform
Abstract
Rationale: The quality and patient-centeredness of intensive care unit (ICU)-based palliative care delivery is highly variable.
Objective: To develop and pilot an app platform for clinicians and ICU patients and their family members that enhances the delivery of needs-targeted palliative care.
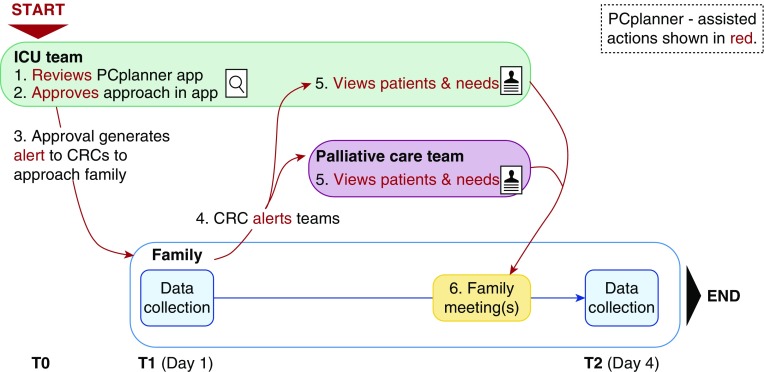
Methods: In the development phase of the study, we developed an electronic health record (EHR) system-integrated mobile web app system prototype, PCplanner (Palliative Care Planner). PCplanner screens the EHR for ICU patients meeting any of five prompts (triggers) for palliative care consultation, allows families to report their unmet palliative care needs, and alerts clinicians to these needs. The evaluation phase included a prospective before/after study conducted at a large academic medical center. Two control populations were enrolled in the before period to serve as context for the intervention. First, 25 ICU patients who received palliative care consults served as patient-level controls. Second, 49 family members of ICU patients who received mechanical ventilation for at least 48 hours served as family-level controls. Afterward, 14 patients, 18 family members, and 10 clinicians participated in the intervention evaluation period. Family member outcomes measured at baseline and 4 days later included acceptability (Client Satisfaction Questionnaire [CSQ]), usability (Systems Usability Scale [SUS]), and palliative care needs, assessed with the adapted needs of social nature, existential concerns, symptoms, and therapeutic interaction (NEST) scale; the Patient-Centeredness of Care Scale (PCCS); and the Perceived Stress Scale (PSS). Patient outcomes included frequency of goal concordant treatment, hospital length of stay, and discharge disposition.
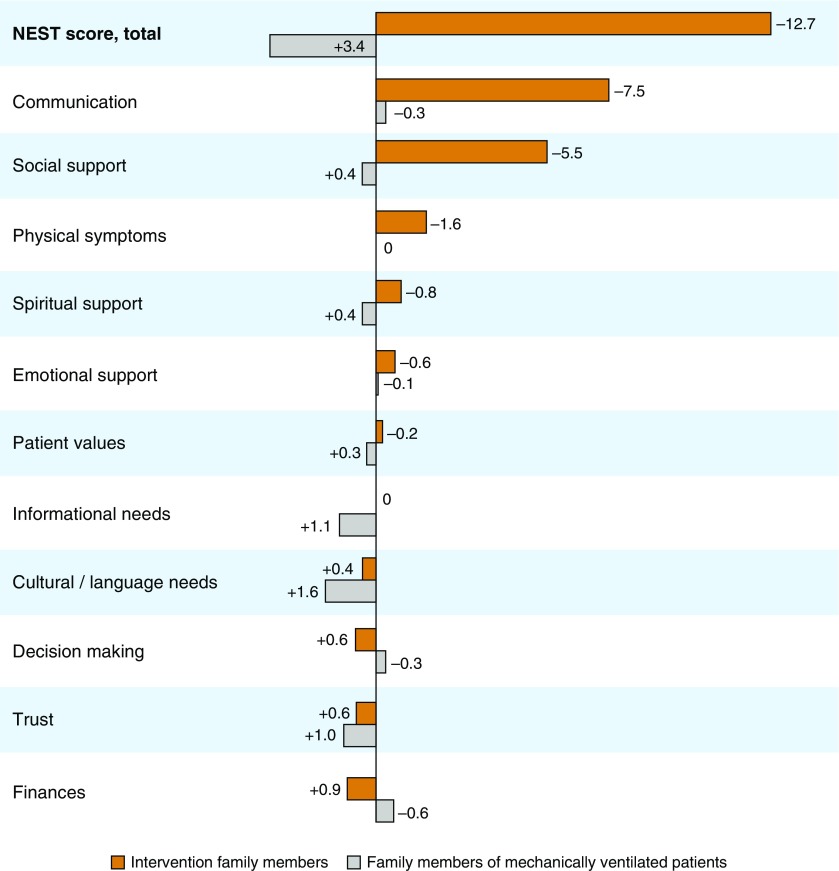
Results: Family members reported high PCplanner acceptability (mean CSQ, 14.1 [SD, 1.4]) and usability (mean SUS, 21.1 [SD, 1.7]). PCplanner family member recipients experienced a 12.7-unit reduction in NEST score compared with a 3.4-unit increase among controls (P = 0.002), as well as improved mean scores on the PCCS (6.6 [SD, 5.8]) and the PSS (-0.8 [SD, 1.9]). The frequency of goal-concordant treatment increased over the course of the intervention (n = 14 [SD, 79%] vs. n = 18 [SD, 100%]). Compared with palliative care controls, intervention patients received palliative care consultation sooner (3.9 [SD, 2.7] vs. 6.9 [SD, 7.1] mean days), had a shorter mean hospital length of stay (20.5 [SD, 9.1] vs. 22.3 [SD, 16.0] patient number), and received hospice care more frequently (5 [36%] vs. 5 [20%]), although these differences were not statistically significant.
Conclusions: PCplanner represents an acceptable, usable, and clinically promising systems-based approach to delivering EHR-triggered, needs-targeted ICU-based palliative care within a standard clinical workflow. A clinical trial in a larger population is needed to evaluate its efficacy.
Keywords: critical illness; electronic health record; palliative care; patient-centeredness; patient-reported outcomes.
Figures
Comment in
-
State-of-the-Art Health Information Technology Meets Patient-centered Care.Ann Am Thorac Soc. 2018 Jan;15(1):18-19. doi: 10.1513/AnnalsATS.201711-840ED. Ann Am Thorac Soc. 2018. PMID: 29286845 No abstract available.
Similar articles
-
Improving racial disparities in unmet palliative care needs among intensive care unit family members with a needs-targeted app intervention: The ICUconnect randomized clinical trial.Contemp Clin Trials. 2021 Apr;103:106319. doi: 10.1016/j.cct.2021.106319. Epub 2021 Feb 13. Contemp Clin Trials. 2021. PMID: 33592310 Free PMC article. Clinical Trial.
-
Operationalizing needs-focused palliative care for older adults in intensive care units: Design of and rationale for the PCplanner randomized clinical trial.Contemp Clin Trials. 2020 Nov;98:106163. doi: 10.1016/j.cct.2020.106163. Epub 2020 Sep 29. Contemp Clin Trials. 2020. PMID: 33007442 Free PMC article. Clinical Trial.
-
Mobile Application-Based Communication Facilitation Platform for Family Members of Critically Ill Patients: A Randomized Clinical Trial.JAMA Netw Open. 2024 Jan 2;7(1):e2349666. doi: 10.1001/jamanetworkopen.2023.49666. JAMA Netw Open. 2024. PMID: 38175648 Free PMC article. Clinical Trial.
-
Easing Suffering for ICU Patients and Their Families: Evidence and Opportunities for Primary and Specialty Palliative Care in the ICU.J Intensive Care Med. 2024 Aug;39(8):715-732. doi: 10.1177/08850666231204305. Epub 2023 Oct 11. J Intensive Care Med. 2024. PMID: 37822226 Review.
-
The changing role of palliative care in the ICU.Crit Care Med. 2014 Nov;42(11):2418-28. doi: 10.1097/CCM.0000000000000573. Crit Care Med. 2014. PMID: 25167087 Free PMC article. Review.
Cited by
-
Mobile App-Facilitated Collaborative Palliative Care Intervention for Critically Ill Older Adults: A Randomized Clinical Trial.JAMA Intern Med. 2025 Feb 1;185(2):173-183. doi: 10.1001/jamainternmed.2024.6838. JAMA Intern Med. 2025. PMID: 39680398 Clinical Trial.
-
Palliative care phenotypes among critically ill patients and family members: intensive care unit prospective cohort study.BMJ Support Palliat Care. 2022 Sep 27:bmjspcare-2022-003622. doi: 10.1136/spcare-2022-003622. Online ahead of print. BMJ Support Palliat Care. 2022. PMID: 36167642 Free PMC article.
-
Palliative Care Early in the Care Continuum among Patients with Serious Respiratory Illness: An Official ATS/AAHPM/HPNA/SWHPN Policy Statement.Am J Respir Crit Care Med. 2022 Sep 15;206(6):e44-e69. doi: 10.1164/rccm.202207-1262ST. Am J Respir Crit Care Med. 2022. PMID: 36112774 Free PMC article.
-
Understanding the Feasibility, Acceptability, and Efficacy of a Clinical Pharmacist-led Mobile Approach (BPTrack) to Hypertension Management: Mixed Methods Pilot Study.J Med Internet Res. 2020 Aug 11;22(8):e19882. doi: 10.2196/19882. J Med Internet Res. 2020. PMID: 32780026 Free PMC article.
-
Improving racial disparities in unmet palliative care needs among intensive care unit family members with a needs-targeted app intervention: The ICUconnect randomized clinical trial.Contemp Clin Trials. 2021 Apr;103:106319. doi: 10.1016/j.cct.2021.106319. Epub 2021 Feb 13. Contemp Clin Trials. 2021. PMID: 33592310 Free PMC article. Clinical Trial.
References
-
- Nelson JE, Meier DE, Litke A, Natale DA, Siegel RE, Morrison RS. The symptom burden of chronic critical illness. Crit Care Med. 2004;32:1527–1534. - PubMed
-
- Angus DC, Barnato AE, Linde-Zwirble WT, Weissfeld LA, Watson RS, Rickert T, et al. Robert Wood Johnson Foundation ICU End-Of-Life Peer Group. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32:638–643. - PubMed
-
- Cook D, Swinton M, Toledo F, Clarke F, Rose T, Hand-Breckenridge T, et al. Personalizing death in the intensive care unit: the 3 Wishes Project: a mixed-methods study. Ann Intern Med. 2015;163:271–279. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
