

Robotic versus laparoscopic distal pancreatectomy: an up-to-date meta-analysis
- PMID: 29121885
- PMCID: PMC5680787
- DOI: 10.1186/s12893-017-0301-3
Robotic versus laparoscopic distal pancreatectomy: an up-to-date meta-analysis
Abstract
Background: Laparoscopic distal pancreatectomy (LDP) reduces postoperative morbidity, hospital stay and recovery as compared with open distal pancreatectomy. Many authors believe that robotic surgery can overcome the difficulties and technical limits of LDP thanks to improved surgical manipulation and better visualization. Few studies in the literature have compared the two methods in terms of surgical and oncological outcome. The aim of this study was to compare the results of robotic (RDP) and laparoscopic distal pancreatectomy.
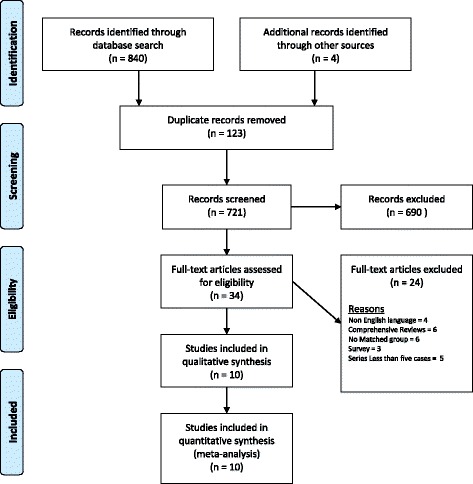
Methods: A systematic review and meta-analysis was conducted of control studies published up to December 2016 comparing LDP and RDP. Two Reviewers independently assessed the eligibility and quality of the studies. The meta-analysis was conducted using either the fixed-effect or the random-effect model.
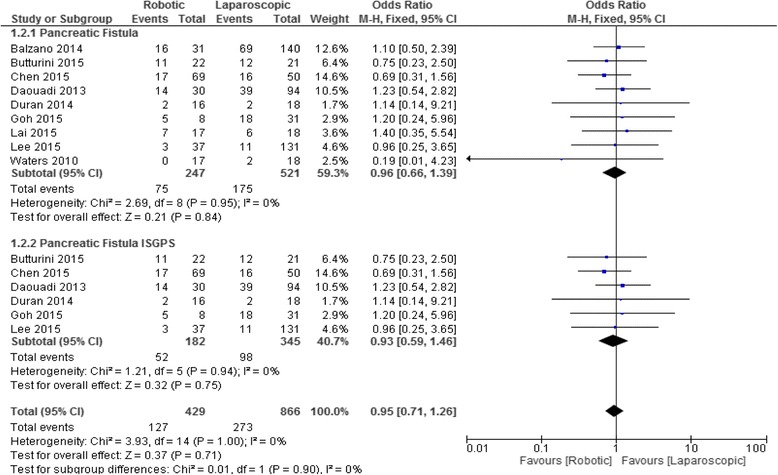
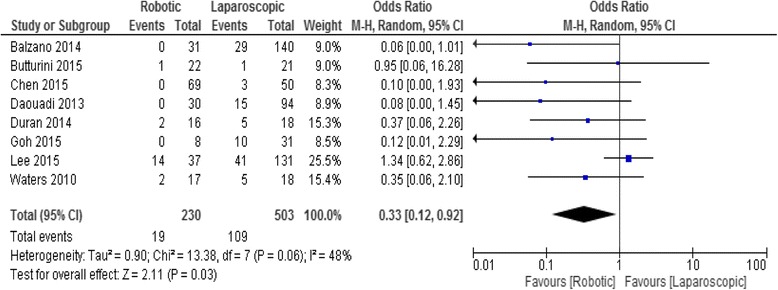
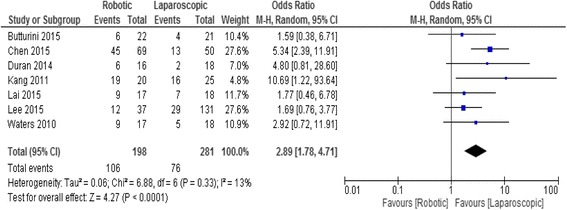
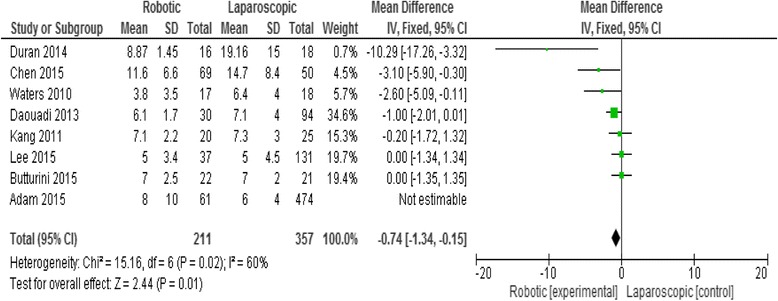
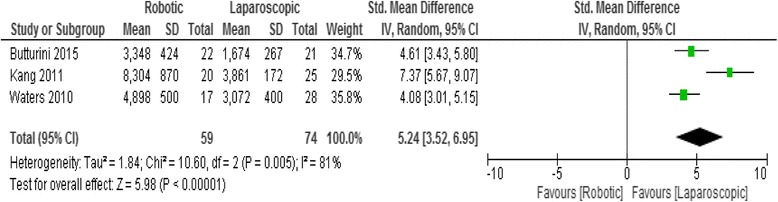
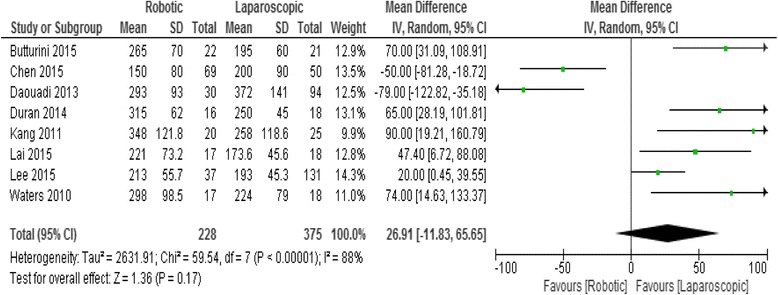
Results: Ten studies describing 813 patients met the inclusion criteria. This meta-analysis shows that the RDP group had a significantly higher rate of spleen preservation [OR 2.89 (95% confidence interval 1.78-4.71, p < 0.0001], a lower rate of conversion to open OR 0.33 (95% CI 0.12-0.92), p = 0.003] and a shorter hospital stay [MD -0.74; (95% CI -1.34 -0.15), p = 0.01] but a higher cost than the LDP group, while other surgical outcomes did not differ between the two groups.
Conclusion: This meta-analysis suggests that the RDP procedure is safe and comparable in terms of surgical results to LDP. However, even if the RDP has a higher cost compared to LDP, it increases the rate of spleen preservation, reduces the risk of conversion to open surgery and is associated to shorter length of hospital stay.
Keywords: Distal pancreatectomy; Laparoscopic surgery; Left pancreatectomy; Meta-analysis; Pancreatic cancer; Pancreatic resection; Review; Robotic surgery.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Wellner UF, Lapshyn H, Bartsch DK, Mintziras I, Hopt UT, Wittel U, Kramling HJ, Preissinger-Heinzel H, Anthuber M, Geissler B, et al. Laparoscopic versus open distal pancreatectomy-a propensity score-matched analysis from the German StuDoQ|pancreas registry. Int J Color Dis. 2017;32(2):273–280. doi: 10.1007/s00384-016-2693-4. - DOI - PubMed
-
- Sulpice L, Farges O, Goutte N, Bendersky N, Dokmak S, Sauvanet A, Delpero JR and ACHBT French Pancreatectomy Study Group. Laparoscopic distal Pancreatectomy for pancreatic Ductal Adenocarcinoma: time for a randomized controlled trial? Results of an all-inclusive National Observational Study. Ann Surg. 2015;262(5):868-73. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
