

Advances and challenges in cirrhosis and portal hypertension
- PMID: 29121925
- PMCID: PMC5680752
- DOI: 10.1186/s12916-017-0966-6
Advances and challenges in cirrhosis and portal hypertension
Abstract
Background: Liver cirrhosis is the fourth cause of death in adults in Western countries, with complications of portal hypertension being responsible for most casualties. In order to reduce mortality, development of accurate diagnostic methods for early diagnosis, effective etiologic treatment, improved pharmacological therapy for portal hypertension, and effective therapies for end-stage liver failure are required.
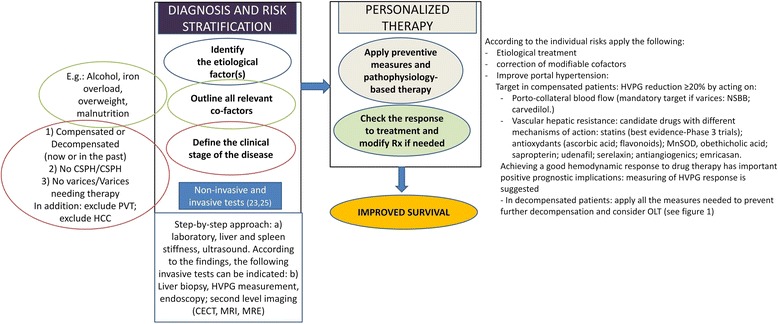
Discussion: Early detection of cirrhosis and portal hypertension is now possible using simple non-invasive methods, leading to the advancement of individualized risk stratification in clinical practice. Despite previous assumptions, cirrhosis can regress if its etiologic cause is effectively removed. Nevertheless, while this is now possible for cirrhosis caused by chronic hepatitis C, the incidence of cirrhosis due to non-alcoholic steatohepatitis has increased dramatically and effective therapies are not yet available. New drugs acting on the dynamic component of hepatic vascular resistance are being studied and will likely improve the future management of portal hypertension.
Conclusion: Cirrhosis is now seen as a dynamic disease able to progress and regress between the compensated and decompensated stages. This opinion article aims to provide the author's personal view of the current major advances and challenges in this field.
Keywords: Hepatic venous pressure gradient; Liver stiffness; Non-invasive methods; Therapy; Transjugular intrahepatic portosystemic shunt.
Conflict of interest statement
Competing interests
The author has no competing interests to disclose.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Agreement between wedged hepatic venous pressure and portal pressure in non-alcoholic steatohepatitis-related cirrhosis.J Hepatol. 2021 Apr;74(4):811-818. doi: 10.1016/j.jhep.2020.10.003. Epub 2020 Oct 14. J Hepatol. 2021. PMID: 33068638
-
Advancing hepatic recompensation: Baveno VII criteria and therapeutic innovations in liver cirrhosis management.World J Gastroenterol. 2024 Jun 21;30(23):2954-2958. doi: 10.3748/wjg.v30.i23.2954. World J Gastroenterol. 2024. PMID: 38946869 Free PMC article. Review.
-
CXCL9 is a prognostic marker in patients with liver cirrhosis receiving transjugular intrahepatic portosystemic shunt.J Hepatol. 2015 Feb;62(2):332-9. doi: 10.1016/j.jhep.2014.09.032. Epub 2014 Oct 17. J Hepatol. 2015. PMID: 25457205
-
[Follow-up study of 116 cases of transjugular intrahepatic portosystemic shunt in the treatment of cirrhotic portal hypertension].Zhonghua Gan Zang Bing Za Zhi. 2018 Aug 20;26(8):596-600. doi: 10.3760/cma.j.issn.1007-3418.2018.08.007. Zhonghua Gan Zang Bing Za Zhi. 2018. PMID: 30317791 Chinese.
-
Transjugular intrahepatic portosystemic shunt in patients with cirrhosis: Indications and posttransjugular intrahepatic portosystemic shunt complications in 2020.United European Gastroenterol J. 2021 Mar;9(2):203-208. doi: 10.1177/2050640620952637. Epub 2021 Feb 23. United European Gastroenterol J. 2021. PMID: 32819214 Free PMC article. Review.
Cited by
-
Management of Adverse Events Associated with Cabozantinib Treatment in Patients with Advanced Hepatocellular Carcinoma.Target Oncol. 2020 Aug;15(4):549-565. doi: 10.1007/s11523-020-00736-8. Target Oncol. 2020. PMID: 32770441 Free PMC article.
-
Multiparametric ultrasound as a new concept of assessment of liver tissue damage.World J Gastroenterol. 2024 Mar 28;30(12):1663-1669. doi: 10.3748/wjg.v30.i12.1663. World J Gastroenterol. 2024. PMID: 38617743 Free PMC article.
-
Clinical Outcomes of Metastatic Breast Cancer in Patients Having Imaging Liver Pseudocirrhosis with or without Evident Varices.Oncologist. 2022 Dec 9;27(12):1008-1015. doi: 10.1093/oncolo/oyac199. Oncologist. 2022. PMID: 36215276 Free PMC article.
-
No Benefit of Hemostatic Drugs on Acute Upper Gastrointestinal Bleeding in Cirrhosis.Biomed Res Int. 2020 Jun 26;2020:4097170. doi: 10.1155/2020/4097170. eCollection 2020. Biomed Res Int. 2020. PMID: 32685481 Free PMC article.
-
Hepatic Veno-Occlusive Disease and Colorectal Cancer: Expect the Unexpected.Life (Basel). 2024 Jul 4;14(7):845. doi: 10.3390/life14070845. Life (Basel). 2024. PMID: 39063599 Free PMC article.
References
-
- Mortality GBD, Mortality GBD, Causes of Death C Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385:117–171. doi: 10.1016/S0140-6736(14)61682-2. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
