

The Diagnosis of Chronic Coronary Heart Disease
- PMID: 29122104
- PMCID: PMC5686296
- DOI: 10.3238/arztebl.2017.0712
The Diagnosis of Chronic Coronary Heart Disease
Abstract
Background: Chronic coronary heart disease (CHD) and acute myocardial infarction are endemic conditions. In Germany, an estimated 900 000 cardiac catheterizations were performed in the year 2014, and a percutaneous intervention was carried out in 40% of these procedures. It would be desirable to lessen the number of invasive diagnostic procedures while preserving the reliability of diagnosis. In this article, we present the updated recommendations of the German National Care Guideline for Chronic CHD with regard to diagnostic evaluation.
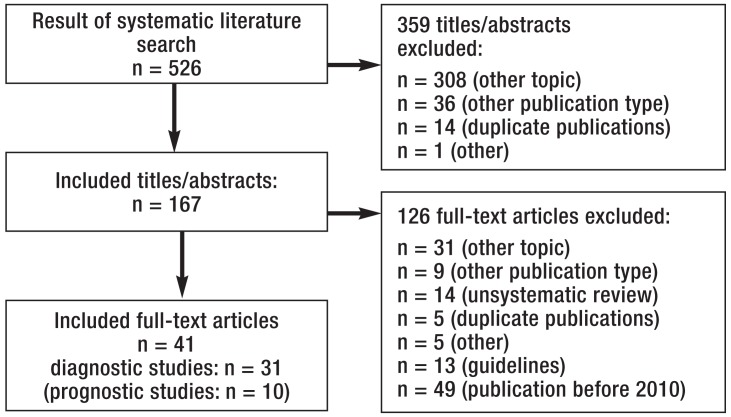
Methods: Updated recommendations for the diagnostic evaluation of chronic CHD were developed on the basis of existing guidelines and a systematic literature review and approved by a formal consensus process.
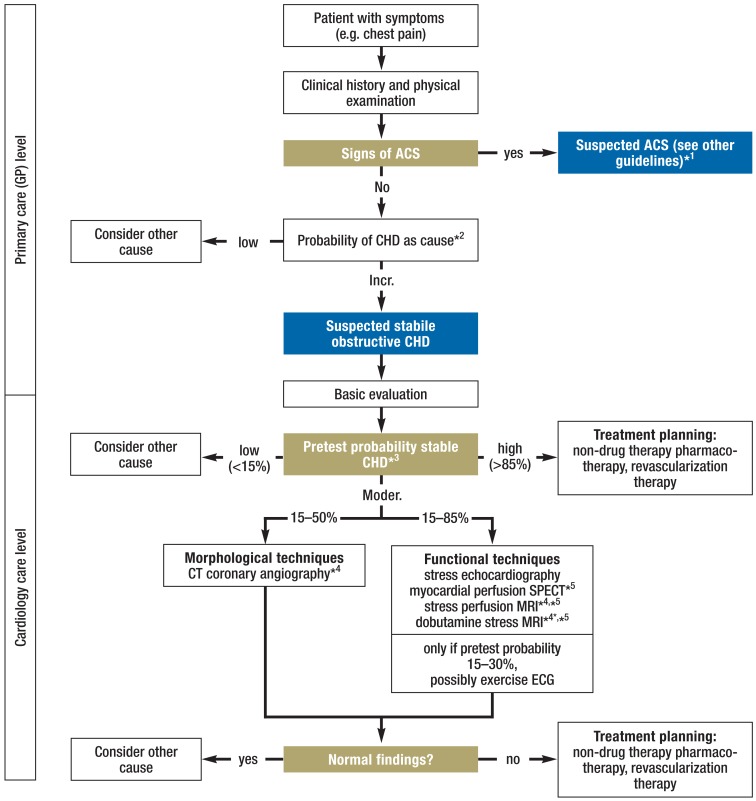
Results: 8-11% of patients with chest pain who present to a general practitioner and 20-25% of those who present to a cardiologist have chronic CHD. General practitioners should estimate the probability of CHD with the Marburg Heart Score. Specialists can use detailed tables for determining the pre-test probability of CHD; if this lies in the range of 15% to 85%, then non-invasive tests should be primarily used for evaluation and treatment planning. If the pretest probability is less than 15%, other potential causes should be ruled out first. If it is over 85%, the presence of CHD should be presumed and treatment planning should be initiated. Coronary angiography is needed only if therapeutic implications are expected (revascularization). Psychosocial risk factors for the development and course of CHD and the patient's quality of life should be regularly assessed as well.
Conclusion: Non-invasive testing and invasive coronary angiography should be used only if their findings are expected to have therapeutic implications. Psychosocial risk factors, the quality of life, and adherence to treatment are important components of these patients' diagnostic evaluation and long-term care.
Figures
Comment in
-
The Importance of Ergometry Was Underrated.Dtsch Arztebl Int. 2018 Feb 23;115(8):131. doi: 10.3238/arztebl.2018.0131a. Dtsch Arztebl Int. 2018. PMID: 29526185 Free PMC article. No abstract available.
-
Current Clinical Practice Is Different.Dtsch Arztebl Int. 2018 Feb 23;115(8):131. doi: 10.3238/arztebl.2018.0131b. Dtsch Arztebl Int. 2018. PMID: 29526186 Free PMC article. No abstract available.
-
Limitations of the Study.Dtsch Arztebl Int. 2018 Feb 23;115(8):133. doi: 10.3238/arztebl.2018.0133a. Dtsch Arztebl Int. 2018. PMID: 29526188 Free PMC article. No abstract available.
-
Incomplete and Curtailed Statements.Dtsch Arztebl Int. 2018 Feb 23;115(8):133-134. doi: 10.3238/arztebl.2018.0133b. Dtsch Arztebl Int. 2018. PMID: 29526189 Free PMC article. No abstract available.
References
-
- Gosswald A, Schienkiewitz A, Nowossadeck E, Busch MA. Prävalenz von Herzinfarkt und koronarer Herzkrankheit bei Erwachsenen im Alter von 40 bis 79 Jahren in Deutschland Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1) Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013;56:650–655. - PubMed
-
- Deutsche Herzstiftung. Deutsche Herzstiftung. Frankfurt/Main: 2016. Deutscher Herzbericht 2016. 28. Sektorenübergreifende Versorgungsanalyse zur Kardiologie und Herzchirurgie in Deutschland.
-
- Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF) Nationale VersorgungsLeitlinie Chronische KHK - Langfassung, 4. Auflage. Version 1. http://doi.org/ 10.6101/AZQ/000267 (last accessed on 26 June 2017) - DOI
-
- Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF) Nationale VersorgungsLeitlinie Chronische KHK - Leitlinienreport, 4. Auflage. Version 1. http://doi.org/ 10.6101/AZQ/000264 (last accessed on 26 June 2017) - DOI
-
- Haasenritter J, Bösner S, Klug J, Ledig T, Donner-Banzhoff N Deutsche Gesellschaft für Allgemeinmedizin und Familienmedizin (DEGAM) Omikron Publ. Düsseldorf: 2011. Brustschmerz. DEGAM-Leitlinie Nr. 15.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources