

Glial function (and dysfunction) in the normal & ischemic brain
- PMID: 29122627
- PMCID: PMC6132239
- DOI: 10.1016/j.neuropharm.2017.11.009
Glial function (and dysfunction) in the normal & ischemic brain
Abstract
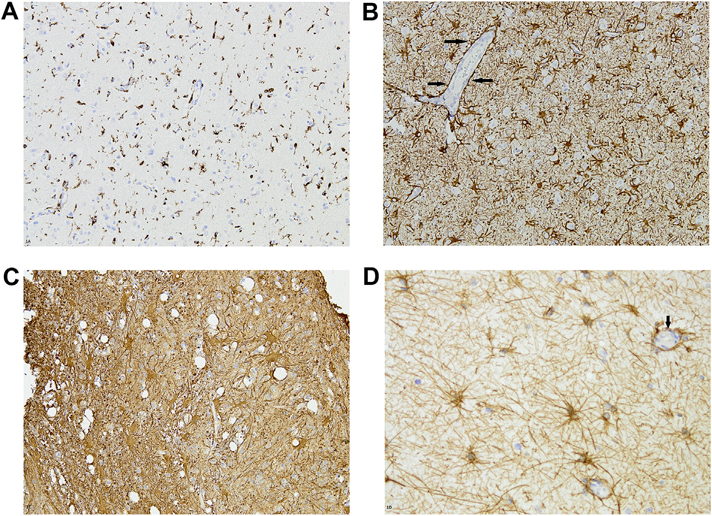
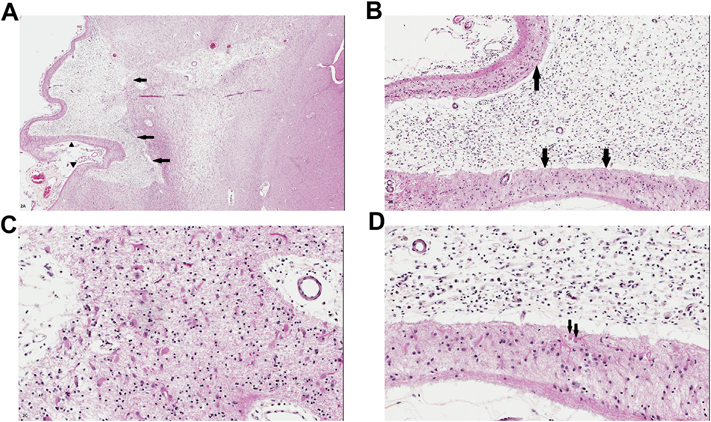
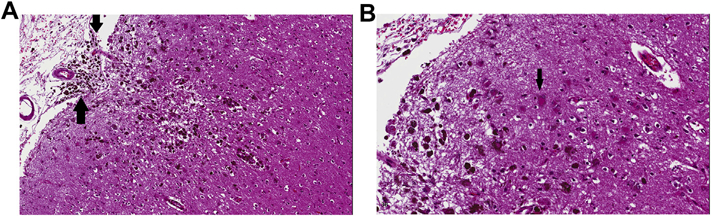
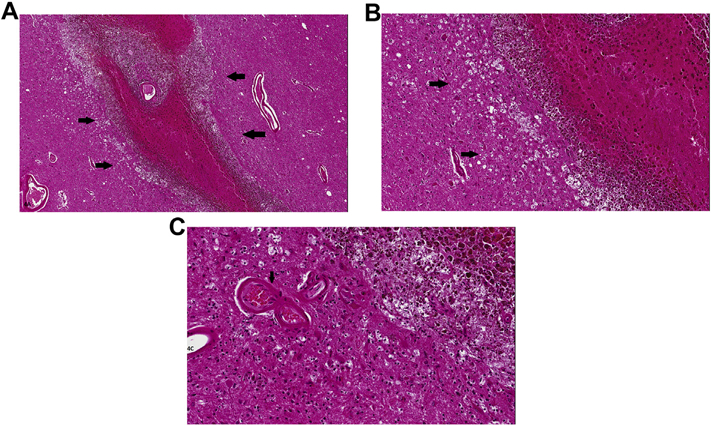
Astrocytes are the most abundant cell type in the central nervous system (CNS). Once considered to be of fairly homogeneous phenotype throughout the brain and spinal cord, they are now understood to be heterogeneous in both structure and function. They are important in brain functions as diverse as ion and fluid balance in the interstitial space, contributing to integrity of the neurovascular unit (blood-brain barrier), neurotransmitter regulation, metabolism of energy substrates and possibly even axonal regeneration. After ischemic or hemorrhagic brain/spinal cord injury, formation of an astrocytic scar adjacent to the 'lesion' is a characteristic histopathologic feature, and this astrogliosis can be demonstrated by immunohistochemistry, usually using primary antibodies to glial fibrillary acidic protein (GFAP). Astrocytes interact with microglia and oligodendroglia in novel ways that will be discussed in this review. This article is part of the Special Issue entitled 'Cerebral Ischemia'.
Keywords: Astrocytes; Brain injury - responses; Intracerebral hemorrhage; Ischemia; Microglia; Oligodendroglia.
Copyright © 2017 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Astrocyte-Derived Estrogen Regulates Reactive Astrogliosis and is Neuroprotective following Ischemic Brain Injury.J Neurosci. 2020 Dec 9;40(50):9751-9771. doi: 10.1523/JNEUROSCI.0888-20.2020. Epub 2020 Nov 6. J Neurosci. 2020. PMID: 33158962 Free PMC article.
-
Sevoflurane postconditioning attenuates reactive astrogliosis and glial scar formation after ischemia-reperfusion brain injury.Neuroscience. 2017 Jul 25;356:125-141. doi: 10.1016/j.neuroscience.2017.05.004. Epub 2017 May 10. Neuroscience. 2017. PMID: 28501505
-
Selective knockout of astrocytic Na+ /H+ exchanger isoform 1 reduces astrogliosis, BBB damage, infarction, and improves neurological function after ischemic stroke.Glia. 2018 Jan;66(1):126-144. doi: 10.1002/glia.23232. Epub 2017 Sep 19. Glia. 2018. PMID: 28925083 Free PMC article.
-
Astrogliosis and glial scar in ischemic stroke - focused on mechanism and treatment.Exp Neurol. 2025 Mar;385:115131. doi: 10.1016/j.expneurol.2024.115131. Epub 2024 Dec 27. Exp Neurol. 2025. PMID: 39733853 Review.
-
The dual role of astrocyte activation and reactive gliosis.Neurosci Lett. 2014 Apr 17;565:30-8. doi: 10.1016/j.neulet.2013.12.071. Epub 2014 Jan 7. Neurosci Lett. 2014. PMID: 24406153 Review.
Cited by
-
Age and Sex Are Critical Factors in Ischemic Stroke Pathology.Endocrinology. 2018 Aug 1;159(8):3120-3131. doi: 10.1210/en.2018-00465. Endocrinology. 2018. PMID: 30010821 Free PMC article. Review.
-
Evaluation of Traumatic Spinal Cord Injury in a Rat Model Using 99mTc-GA-5 as a Potential In Vivo Tracer.Molecules. 2021 Nov 25;26(23):7138. doi: 10.3390/molecules26237138. Molecules. 2021. PMID: 34885718 Free PMC article.
-
Neuropathologic Findings in Elderly HIV-Positive Individuals.J Neuropathol Exp Neurol. 2022 Jun 20;81(7):565-576. doi: 10.1093/jnen/nlac040. J Neuropathol Exp Neurol. 2022. PMID: 35656871 Free PMC article.
-
Regulation of glutamate transport and neuroinflammation in a term newborn rat model of hypoxic-ischaemic brain injury.Brain Neurosci Adv. 2022 May 20;6:23982128221097568. doi: 10.1177/23982128221097568. eCollection 2022 Jan-Dec. Brain Neurosci Adv. 2022. PMID: 35615059 Free PMC article.
-
Neuroprotective effects of EpoL against oxidative stress induced by soluble oligomers of Aβ peptide.Redox Biol. 2019 Jun;24:101187. doi: 10.1016/j.redox.2019.101187. Epub 2019 Apr 2. Redox Biol. 2019. PMID: 30965198 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
