

Performance of a Mobile Phone App-Based Participatory Syndromic Surveillance System for Acute Febrile Illness and Acute Gastroenteritis in Rural Guatemala
- PMID: 29122738
- PMCID: PMC5701088
- DOI: 10.2196/jmir.8041
Performance of a Mobile Phone App-Based Participatory Syndromic Surveillance System for Acute Febrile Illness and Acute Gastroenteritis in Rural Guatemala
Abstract
Background: With their increasing availability in resource-limited settings, mobile phones may provide an important tool for participatory syndromic surveillance, in which users provide symptom data directly into a centralized database.
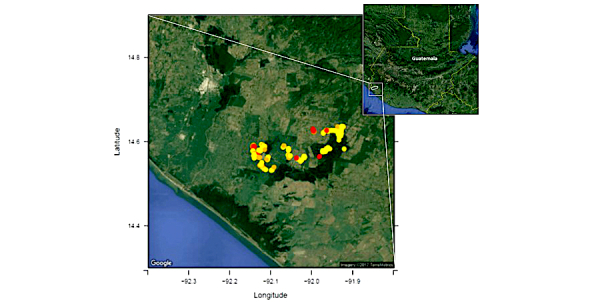
Objective: We studied the performance of a mobile phone app-based participatory syndromic surveillance system for collecting syndromic data (acute febrile illness and acute gastroenteritis) to detect dengue virus and norovirus on a cohort of children living in a low-resource and rural area of Guatemala.
Methods: Randomized households were provided with a mobile phone and asked to submit weekly reports using a symptom diary app (Vigilant-e). Participants reporting acute febrile illness or acute gastroenteritis answered additional questions using a decision-tree algorithm and were subsequently visited at home by a study nurse who performed a second interview and collected samples for dengue virus if confirmed acute febrile illness and norovirus if acute gastroenteritis. We analyzed risk factors associated with decreased self-reporting of syndromic data using the Vigilant-e app and evaluated strategies to improve self-reporting. We also assessed agreement between self-report and nurse-collected data obtained during home visits.
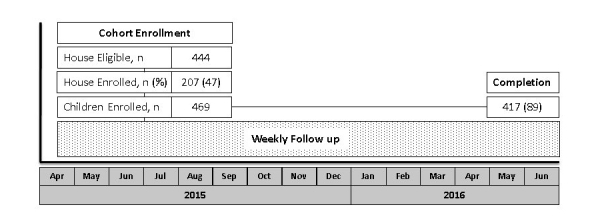
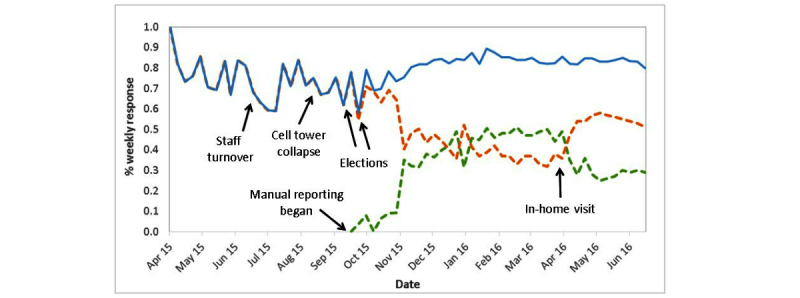
Results: From April 2015 to June 2016, 469 children in 207 households provided 471 person-years of observation. Mean weekly symptom reporting rate was 78% (range 58%-89%). Households with a poor (<70%) weekly reporting rate using the Vigilant-e app during the first 25 weeks of observation (n=57) had a greater number of children (mean 2.8, SD 1.5 vs mean 2.5, SD 1.3; risk ratio [RR] 1.2, 95% CI 1.1-1.4), were less likely to have used mobile phones for text messaging at study enrollment (61%, 35/57 vs 76.7%, 115/150; RR 0.6, 95% CI 0.4-0.9), and were less likely to access care at the local public clinic (35%, 20/57 vs 67.3%, 101/150; RR 0.4, 95% CI 0.2-0.6). Parents of female enrolled participants were more likely to have low response rate (57.1%, 84/147 vs 43.8%, 141/322; RR 1.4, 95% CI 1.1-1.9). Several external factors (cellular tower collapse, contentious elections) were associated with periods of decreased reporting. Poor response rate (<70%) was associated with lower case reporting of acute gastroenteritis, norovirus-associated acute gastroenteritis, acute febrile illness, and dengue virus-associated acute febrile illness (P<.001). Parent-reported syndromic data on the Vigilant-e app demonstrated agreement with nurse-collected data for fever (kappa=.57, P<.001), vomiting (kappa=.63, P<.001), and diarrhea (kappa=.61, P<.001), with decreased agreement as the time interval between parental report and nurse home visit increased (<1 day: kappa=.65-.70; ≥2 days: kappa=.08-.29).
Conclusions: In a resource-limited area of rural Guatemala, a mobile phone app-based participatory syndromic surveillance system demonstrated a high reporting rate and good agreement between parental reported data and nurse-reported data during home visits. Several household-level and external factors were associated with decreased syndromic reporting. Poor reporting rate was associated with decreased syndromic and pathogen-specific case ascertainment.
Keywords: Guatemala; acute febrile illness; app; dengue; diarrhea; mobile phone; norovirus; participatory; syndromic surveillance.
©Daniel Olson, Molly Lamb, Maria Renee Lopez, Kathryn Colborn, Alejandra Paniagua-Avila, Alma Zacarias, Ricardo Zambrano-Perilla, Sergio Ricardo Rodríguez-Castro, Celia Cordon-Rosales, Edwin Jose Asturias. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 09.11.2017.
Conflict of interest statement
Conflicts of Interest: Dr Asturias has served on an Advisory Board for Takeda Vaccines Inc and is partially supported by research grants from GlaxoSmithKline Biologicals and Takeda Vaccines Inc. Dr Lamb is partially supported by grants from GlaxoSmithKline Biologicals and Pantheryx Inc. Dr Olson is partially supported by a grant from Takeda Vaccines Inc. Ricardo Zambrano-Perilla and Sergio Ricardo Rodríguez-Castro are employed by Integra IT and own stake in the company.
Figures
References
-
- Li Y, Fang L, Gao S, Wang Z, Gao H, Liu P, Wang Z, Li Y, Zhu X, Li X, Xu B, Li Y, Yang H, de Vlas SJ, Shi T, Cao W. Decision support system for the response to infectious disease emergencies based on WebGIS and mobile services in China. PLoS One. 2013;8(1):e54842. doi: 10.1371/journal.pone.0054842. http://dx.plos.org/10.1371/journal.pone.0054842 - DOI - PMC - PubMed
-
- Yang C, Yang J, Luo X, Gong P. Use of mobile phones in an emergency reporting system for infectious disease surveillance after the Sichuan earthquake in China. Bull World Health Organ. 2009 Aug;87(8):619–623. http://www.scielosp.org/scielo.php?script=sci_arttext&pid=S0042-96862009... - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
