

A nationwide population-based cohort study of peripartum hysterectomy and arterial embolisation in Belgium: results from the Belgian Obstetric Surveillance System
- PMID: 29122786
- PMCID: PMC5695365
- DOI: 10.1136/bmjopen-2017-016208
A nationwide population-based cohort study of peripartum hysterectomy and arterial embolisation in Belgium: results from the Belgian Obstetric Surveillance System
Abstract
Objectives: To assess the prevalence of major obstetric haemorrhage managed with peripartum hysterectomy and/or interventional radiology (IR) in Belgium. To describe women characteristics, the circumstances in which the interventions took place, the management of the obstetric haemorrhage, the outcome and additional morbidity of these women.
Design: Nationwide population-based prospective cohort study.
Setting: Emergency obstetric care. Participation of 97% of maternities covering 98.6% of deliveries in Belgium.
Participants: All women who underwent peripartum hysterectomy and/or IR procedures in Belgium between January 2012 and December 2013.
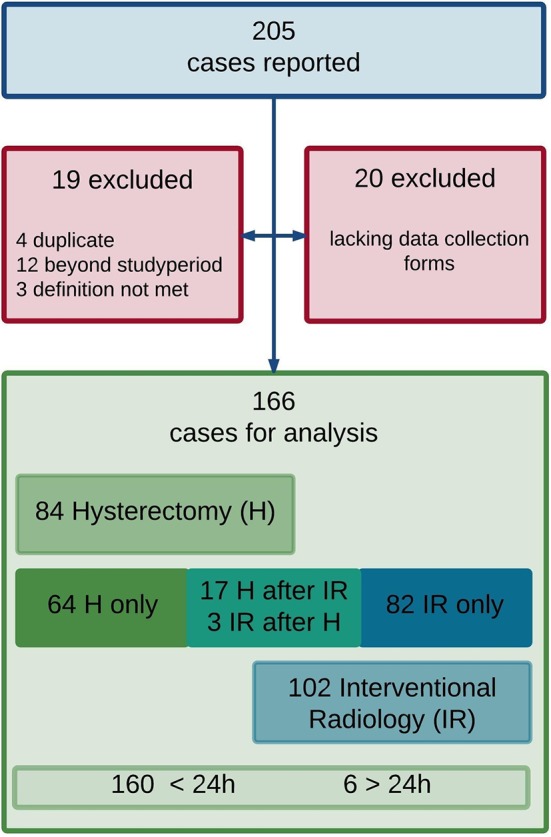
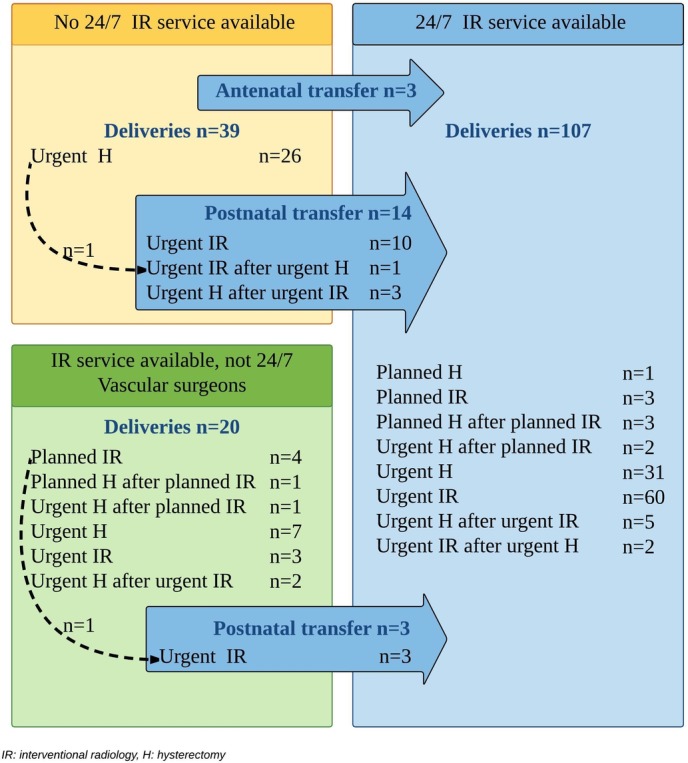
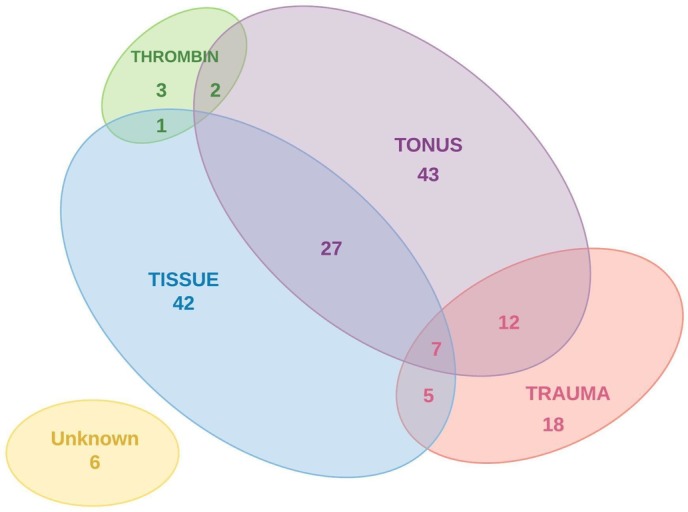
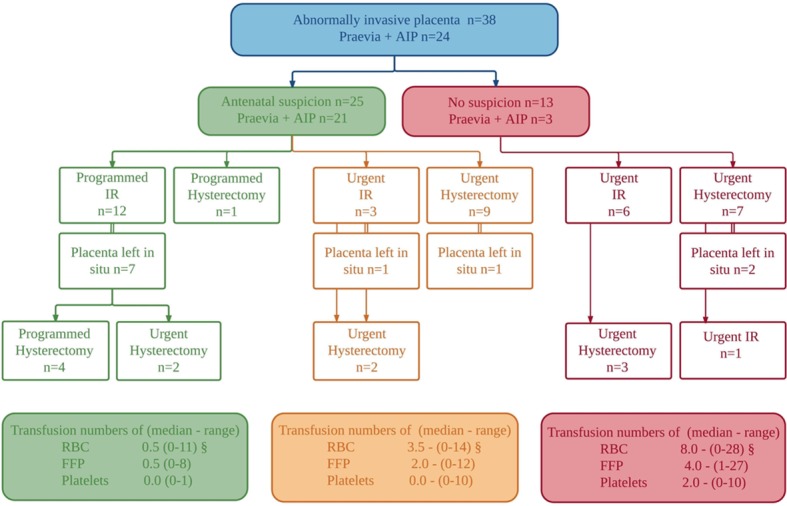
Results: We obtained data on 166 women who underwent peripartum hysterectomy (n=84) and/or IR procedures (n=102), corresponding to 1 in 3030 women undergoing a peripartum hysterectomy and another 1 in 3030 women being managed by IR, thereby preserving the uterus. Seventeen women underwent hysterectomy following IR and three women needed further IR despite hysterectomy. Abnormal placentation and/or uterine atony were the reported causes of haemorrhage in 83.7%. Abnormally invasive placenta was not detected antenatally in 34% of cases. The interventions were planned in 15 women. Three women were transferred antenatally and 17 women postnatally to a hospital with emergency IR service. Urgent peripartum hysterectomy was averted in 72% of the women who were transferred, with no significant difference in need for transfusion. IR procedures were able to stop the bleeding in 87.8% of the attempts. Disseminated intravascular coagulation secondary to major haemorrhage was reported in 32 women (19%).
Conclusion: The prevalence in Belgium of major obstetric haemorrhage requiring peripartum hysterectomy and/or IR is estimated at 6.6 (95% CI 5.7 to 7.7) per 10 000 deliveries. Increased clinician awareness of the risk factors of abnormal placentation could further improve the management and outcome of major obstetric haemorrhage. A case-by-case in-depth analysis is necessary to reveal whether the hysterectomies and arterial embolisations performed in this study were appropriate or preventable.
Keywords: arterial embolisation; interventional radiology; major obstetrichaemorrhage; maternal near miss; peripartum hysterectomy; severe maternal morbidity.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and hereby declare that they have no financial relationships with any organisations that might have an interest in the submitted work in the past 3 years, nor that they have partaken of any other relationships or activities that could appear to have influenced the submitted work.
Figures
Similar articles
-
Management of major obstetric hemorrhage prior to peripartum hysterectomy and outcomes across nine European countries.Acta Obstet Gynecol Scand. 2021 Jul;100(7):1345-1354. doi: 10.1111/aogs.14113. Epub 2021 Mar 14. Acta Obstet Gynecol Scand. 2021. PMID: 33719032 Free PMC article.
-
Incidence of emergency peripartum hysterectomy in Ain-shams University Maternity Hospital, Egypt: a retrospective study.Arch Gynecol Obstet. 2014 Nov;290(5):891-6. doi: 10.1007/s00404-014-3306-5. Epub 2014 Jun 15. Arch Gynecol Obstet. 2014. PMID: 24930117
-
Analysis of 59 cases of emergent peripartum hysterectomies during a 13-year period.Arch Gynecol Obstet. 2005 Apr;271(4):363-7. doi: 10.1007/s00404-004-0647-5. Epub 2004 Jun 15. Arch Gynecol Obstet. 2005. PMID: 15205986
-
[Intractable postpartum haemorrhages: where is the place of vascular ligations, emergency peripartum hysterectomy or arterial embolization?].Gynecol Obstet Fertil. 2004 Apr;32(4):320-9. doi: 10.1016/j.gyobfe.2004.02.003. Gynecol Obstet Fertil. 2004. PMID: 15123103 Review. French.
-
Incidence, Indications, Risk Factors, and Outcomes of Emergency Peripartum Hysterectomy Worldwide: A Systematic Review and Meta-analysis.Obstet Gynecol. 2023 Jan 1;141(1):35-48. doi: 10.1097/AOG.0000000000005022. Epub 2022 Nov 30. Obstet Gynecol. 2023. PMID: 36701608
Cited by
-
Uterine Factor Infertility, a Systematic Review.J Clin Med. 2022 Aug 21;11(16):4907. doi: 10.3390/jcm11164907. J Clin Med. 2022. PMID: 36013146 Free PMC article. Review.
-
Placenta Accreta Spectrum Leading to Peripartum Hysterectomy: A Case Report.Cureus. 2025 Apr 30;17(4):e83253. doi: 10.7759/cureus.83253. eCollection 2025 Apr. Cureus. 2025. PMID: 40453288 Free PMC article.
-
Epidemiological analysis of peripartum hysterectomy across nine European countries.Acta Obstet Gynecol Scand. 2020 Oct;99(10):1364-1373. doi: 10.1111/aogs.13892. Epub 2020 May 21. Acta Obstet Gynecol Scand. 2020. PMID: 32358968 Free PMC article.
-
Interventional radiology for prevention and management of postpartum haemorrhage: a single centre retrospective cohort study.Arch Gynecol Obstet. 2025 Feb;311(2):251-258. doi: 10.1007/s00404-024-07595-y. Epub 2024 Jun 16. Arch Gynecol Obstet. 2025. PMID: 38879856 Free PMC article.
-
Management of major obstetric hemorrhage prior to peripartum hysterectomy and outcomes across nine European countries.Acta Obstet Gynecol Scand. 2021 Jul;100(7):1345-1354. doi: 10.1111/aogs.14113. Epub 2021 Mar 14. Acta Obstet Gynecol Scand. 2021. PMID: 33719032 Free PMC article.
References
-
- Evaluating the quality of care for severe pregnancy complications: the WHO near-miss approach for maternal health. Switzerland: Geneva, 2011. Retrieved fromAccessed http://apps.who.int/iris/bitstream/10665/44692/1/9789241502221_eng.pdf.
-
- Stones W, Lim W, Al-Azzawi F, et al. . An investigation of maternal morbidity with identification of life-threatening ’near miss' episodes. Health Trends 1991;23:13–15. - PubMed
-
- Lewis G. The Confidential Enquiry into Maternal and Child Health (CEMACH). Saving Mother’s Lives: reviewing maternal deaths to make motherhood safer-2003-2005. The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom. London: CEMACH, 2007.
-
- In: Knight M, Tuffnell D, Kenyon S, Kenyon S, Shakespear J, Gray R, Kurinczuk JJ, et al. eds On behalf of MBRRACE-UK. saving lives, improving mother’s Care - Surveillance of maternal deaths in the UK 2011-13 and lessons learned to inform maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2009-13. Oxford: National Perinatal Epidemiology Unit, University of Oxford, 2015.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical