

Impact of prenatal diagnosis on survival of newborns with four congenital heart defects: a prospective, population-based cohort study in France (the EPICARD Study)
- PMID: 29122798
- PMCID: PMC5695380
- DOI: 10.1136/bmjopen-2017-018285
Impact of prenatal diagnosis on survival of newborns with four congenital heart defects: a prospective, population-based cohort study in France (the EPICARD Study)
Abstract
Objectives: (1) Assess the population-level probability of prenatal diagnosis and termination of pregnancy for fetal anomaly for four major congenital heart defects; (2) Examine, using population-based data, the relation between timing of (prenatal vs postnatal) diagnosis and risk of infant (ie, < 1 year) mortality for four major congenital heart defects (CHDs).
Design: Population-based cohort (the EPIdémiologie des CARDiopathies congénitales) study.
Setting: Greater Paris area (Paris and its surrounding suburbs).
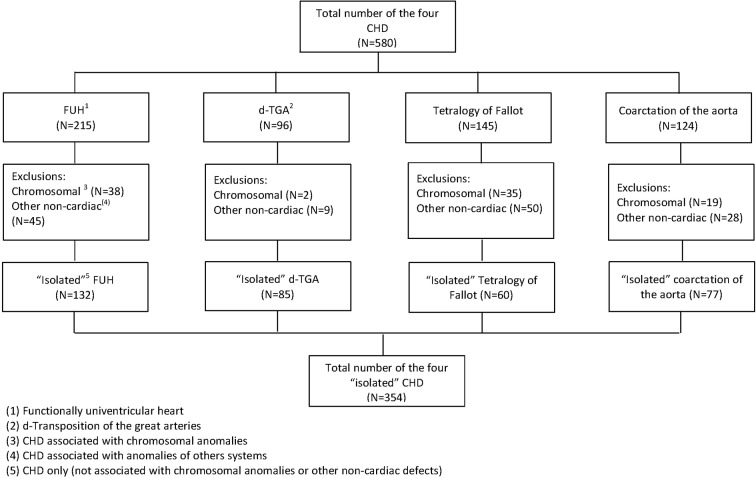
Patients: Three hundred and fifty-four cases of four major CHDs, including functionally univentricular heart (FUH, N=132), d-transposition of great arteries (d-TGA, N=85), tetralogy of Fallot (TOF, N=60) and coarctation of aorta (CoA, N=77). Statistical analysis included the Mantel-Haenszel method and a test of homogeneity of risk ratios.
Results: Approximately 95% of FUH, more than two-thirds of d-TGA and TOF, and 40% of CoA were prenatally diagnosed. Overall, we did not find any statistically significant association between timing of (prenatal vs postnatal) diagnosis of CHD and risk of infant mortality (Mantel-Haenszel risk ratio 1.1, 95% CI 0.5 - 2.7); and the differences between the risk ratios of the association between prenatal diagnosis and infant mortality across the four CHDs was not statistically significant.
Conclusion: These results imply that at least in the settings where specialised services are readily available, survival may no longer be the most relevant outcome, or the best criterion, for evaluating the impact of prenatal diagnosis on the outcome of CHD. The beneficial effects of prenatal diagnosis may be better sought by looking at more 'subtle' or long-term neurodevelopmental outcomes.
Keywords: congenital heart disease; epidemiology; prenatal diagnosis.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- EUROCAT Central Registry UoU. EUROCAT Special Report: Congenital Heart Defects in Europe 2000-2005. 2009. http://www.eurocat-network.eu/content/Special-Report-CHD.pdf.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical