

Comparison of Inappropriate Shocks and Other Health Outcomes Between Single- and Dual-Chamber Implantable Cardioverter-Defibrillators for Primary Prevention of Sudden Cardiac Death: Results From the Cardiovascular Research Network Longitudinal Study of Implantable Cardioverter-Defibrillators
- PMID: 29122811
- PMCID: PMC5721776
- DOI: 10.1161/JAHA.117.006937
Comparison of Inappropriate Shocks and Other Health Outcomes Between Single- and Dual-Chamber Implantable Cardioverter-Defibrillators for Primary Prevention of Sudden Cardiac Death: Results From the Cardiovascular Research Network Longitudinal Study of Implantable Cardioverter-Defibrillators
Abstract
Background: In US clinical practice, many patients who undergo placement of an implantable cardioverter-defibrillator (ICD) for primary prevention of sudden cardiac death receive dual-chamber devices. The superiority of dual-chamber over single-chamber devices in reducing the risk of inappropriate ICD shocks in clinical practice has not been established. The objective of this study was to compare risk of adverse outcomes, including inappropriate shocks, between single- and dual-chamber ICDs for primary prevention.
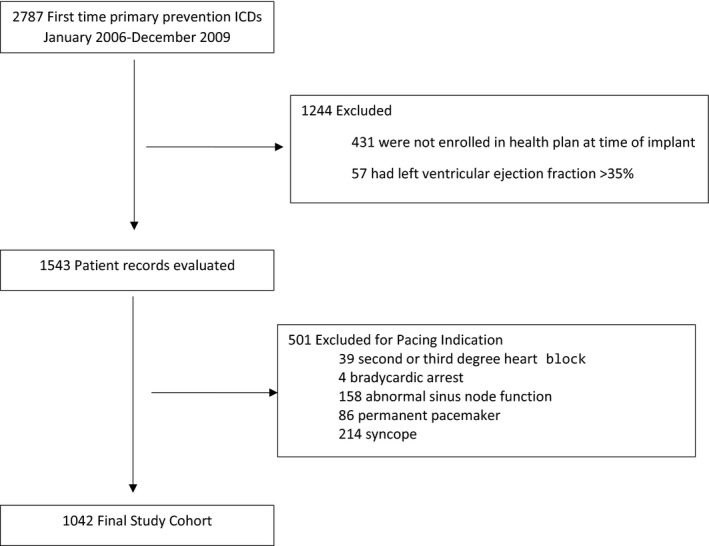
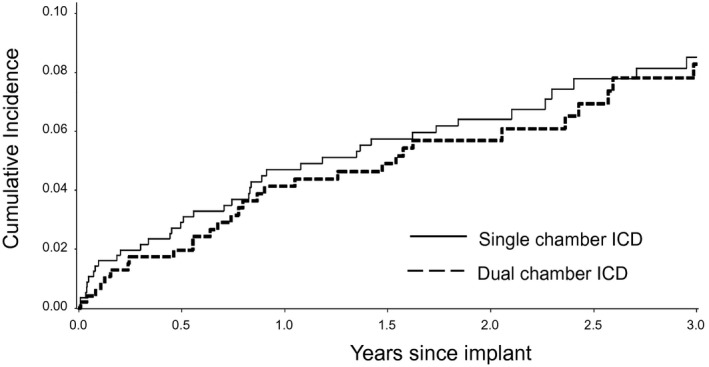
Methods and results: We identified patients receiving a single- or dual-chamber ICD for primary prevention who did not have an indication for pacing from 15 hospitals within 7 integrated health delivery systems in the Longitudinal Study of Implantable Cardioverter-Defibrillators from 2006 to 2009. The primary outcome was time to first inappropriate shock. ICD shocks were adjudicated for appropriateness. Other outcomes included all-cause hospitalization, heart failure hospitalization, and death. Patient, clinician, and hospital-level factors were accounted for using propensity score weighting methods. Among 1042 patients without pacing indications, 54.0% (n=563) received a single-chamber device and 46.0% (n=479) received a dual-chamber device. In a propensity-weighted analysis, device type was not significantly associated with inappropriate shock (hazard ratio, 0.91; 95% confidence interval, 0.59-1.38 [P=0.65]), all-cause hospitalization (hazard ratio, 1.03; 95% confidence interval, 0.87-1.21 [P=0.76]), heart failure hospitalization (hazard ratio, 0.93; 95% confidence interval, 0.72-1.21 [P=0.59]), or death (hazard ratio, 1.19; 95% confidence interval, 0.93-1.53 [P=0.17]).
Conclusions: Among patients who received an ICD for primary prevention without indications for pacing, dual-chamber devices were not associated with lower risk of inappropriate shock or differences in hospitalization or death compared with single-chamber devices. This study does not justify the use of dual-chamber devices to minimize inappropriate shocks.
Keywords: defibrillator shocks; implantable cardioverter‐defibrillators; outcomes research.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Similar articles
-
Single-brand dual-chamber discriminators to prevent inappropriate shocks in patients implanted with prophylactic implantable cardioverter defibrillators: a propensity-weighted comparison of single- and dual-chamber devices.J Interv Card Electrophysiol. 2019 Apr;54(3):267-275. doi: 10.1007/s10840-018-0494-0. Epub 2018 Dec 6. J Interv Card Electrophysiol. 2019. PMID: 30523511
-
A prospective randomized trial of single- or dual-chamber implantable cardioverter-defibrillators to minimize inappropriate shock risk in primary sudden cardiac death prevention.Europace. 2014 Oct;16(10):1460-8. doi: 10.1093/europace/euu022. Epub 2014 Jun 13. Europace. 2014. PMID: 24928948 Clinical Trial.
-
Low inappropriate shock rates in patients with single- and dual/triple-chamber implantable cardioverter-defibrillators using a novel suite of detection algorithms: PainFree SST trial primary results.Heart Rhythm. 2015 May;12(5):926-36. doi: 10.1016/j.hrthm.2015.01.017. Epub 2015 Jan 28. Heart Rhythm. 2015. PMID: 25637563 Clinical Trial.
-
Implantable cardioverter-defibrillator shocks: epidemiology, outcomes, and therapeutic approaches.JAMA Intern Med. 2013 May 27;173(10):859-65. doi: 10.1001/jamainternmed.2013.428. JAMA Intern Med. 2013. PMID: 23546173 Review.
-
Important Parameters for Implantable Cardioverter Defibrillator Selection.Card Electrophysiol Clin. 2018 Mar;10(1):145-152. doi: 10.1016/j.ccep.2017.11.015. Card Electrophysiol Clin. 2018. PMID: 29428136 Review.
Cited by
-
Ventricular arrhythmia management in patients with genetic cardiomyopathies.Heart Rhythm O2. 2021 Dec 17;2(6Part B):819-831. doi: 10.1016/j.hroo.2021.10.009. eCollection 2021 Dec. Heart Rhythm O2. 2021. PMID: 34988533 Free PMC article.
-
Trends in Use of Single- vs Dual-Chamber Implantable Cardioverter-Defibrillators Among Patients Without a Pacing Indication, 2010-2018.JAMA Netw Open. 2022 Mar 1;5(3):e223429. doi: 10.1001/jamanetworkopen.2022.3429. JAMA Netw Open. 2022. PMID: 35315917 Free PMC article.
-
Single vs. dual chamber implantable cardioverter-defibrillators or programming of implantable cardioverter-defibrillators in patients without a bradycardia pacing indication: systematic review and meta-analysis.Europace. 2018 Oct 1;20(10):1621-1629. doi: 10.1093/europace/euy183. Europace. 2018. PMID: 30137296 Free PMC article.
-
Arrhythmia Detection in Atrioventricular, Single-Lead, Floating Atrial Dipole ICD Systems Compared with Conventional Single- and Dual-Chamber Defibrillators.J Cardiovasc Dev Dis. 2024 Dec 1;11(12):386. doi: 10.3390/jcdd11120386. J Cardiovasc Dev Dis. 2024. PMID: 39728276 Free PMC article.
-
Electrical manipulation of the failing heart.Heart Fail Rev. 2018 Nov;23(6):885-896. doi: 10.1007/s10741-018-9732-x. Heart Fail Rev. 2018. PMID: 30099646 Review.
References
-
- Dewland TA, Pellegrini CN, Wang Y, Marcus GM, Keung E, Varosy PD. Dual‐chamber implantable cardioverter‐defibrillator selection is associated with increased complication rates and mortality among patients enrolled in the NCDR implantable cardioverter‐defibrillator registry. J Am Coll Cardiol. 2011;58:1007–1013. - PubMed
-
- Peterson PN, Varosy PD, Heidenreich PA, Wang Y, Dewland TA, Curtis JP, Go AS, Greenlee RT, Magid DJ, Normand SL, Masoudi FA. Association of single‐ vs dual‐chamber ICDs with mortality, readmissions, and complications among patients receiving an ICD for primary prevention. JAMA. 2013;309:2025–2034. - PMC - PubMed
-
- Schron EB, Exner DV, Yao Q, Jenkins LS, Steinberg JS, Cook JR, Kutalek SP, Friedman PL, Bubien RS, Page RL, Powell J. Quality of life in the antiarrhythmics versus implantable defibrillators trial: impact of therapy and influence of adverse symptoms and defibrillator shocks. Circulation. 2002;105:589–594. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
