

68Ga-PSMA-11 PET/CT Mapping of Prostate Cancer Biochemical Recurrence After Radical Prostatectomy in 270 Patients with a PSA Level of Less Than 1.0 ng/mL: Impact on Salvage Radiotherapy Planning
- PMID: 29123013
- PMCID: PMC5807533
- DOI: 10.2967/jnumed.117.201749
68Ga-PSMA-11 PET/CT Mapping of Prostate Cancer Biochemical Recurrence After Radical Prostatectomy in 270 Patients with a PSA Level of Less Than 1.0 ng/mL: Impact on Salvage Radiotherapy Planning
Abstract
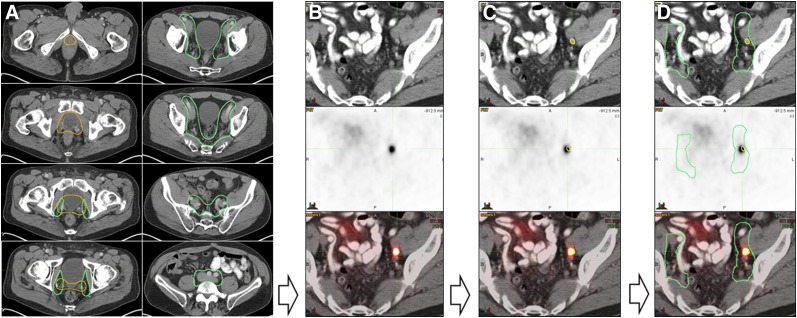
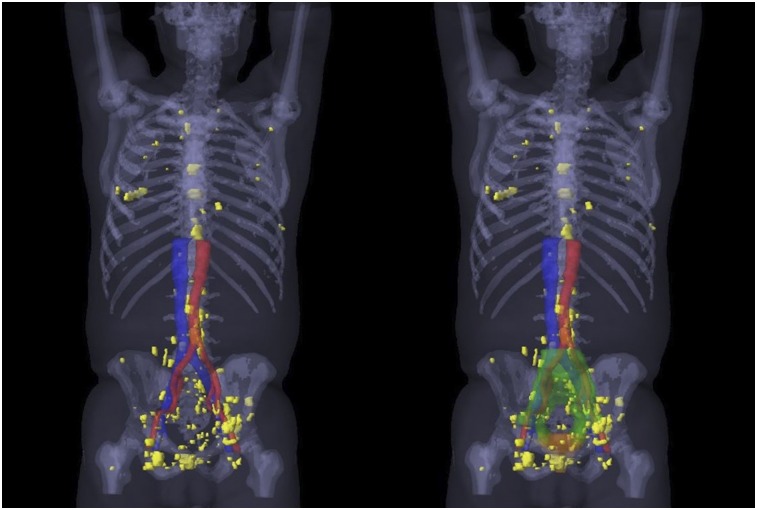
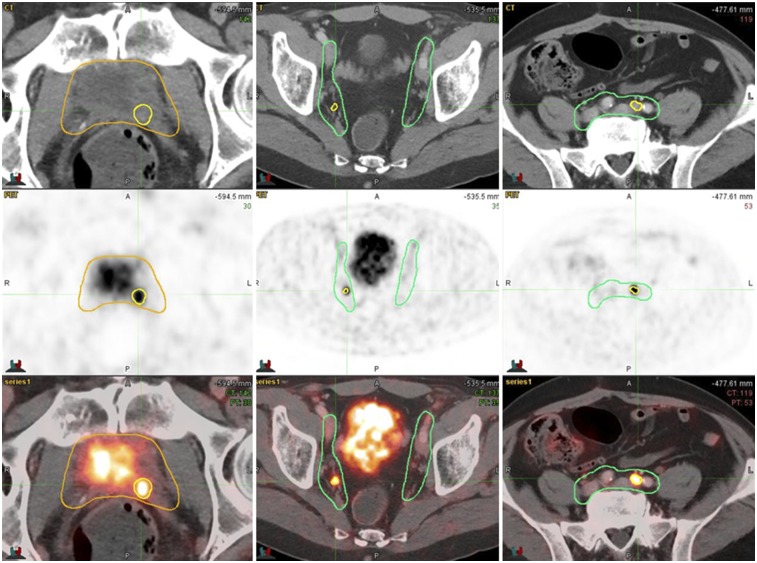
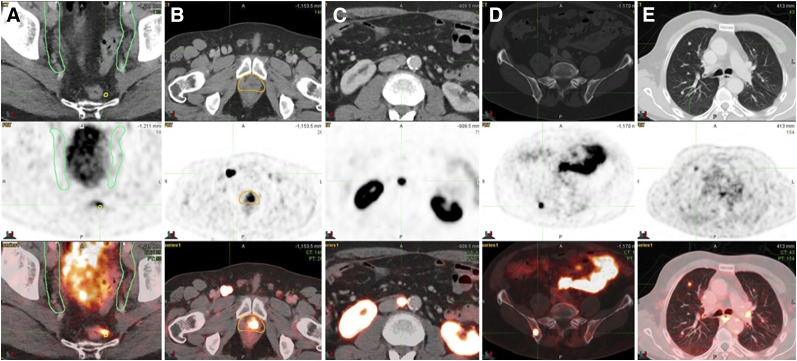
Target volume delineations for prostate cancer (PCa) salvage radiotherapy (SRT) after radical prostatectomy are usually drawn in the absence of visibly recurrent disease. 68Ga-labeled prostate-specific membrane antigen (PSMA-11) PET/CT detects recurrent PCa with sensitivity superior to standard-of-care imaging at serum prostate-specific antigen (PSA) values low enough to affect target volume delineations for routine SRT. Our objective was to map the recurrence pattern of PCa early biochemical recurrence (BCR) after radical prostatectomy with 68Ga-PSMA-11 PET/CT in patients with serum PSA levels of less than 1 ng/mL, determine how often consensus clinical target volumes (CTVs) based on the Radiation Therapy Oncology Group (RTOG) guidelines cover 68Ga-PSMA-11 PET/CT-defined disease, and assess the potential impact of 68Ga-PSMA-11 PET/CT on SRT. Methods: This was a post hoc analysis of an intention-to-treat population of 270 patients who underwent 68Ga-PSMA-11 PET/CT at 4 institutions for BCR after prostatectomy without prior radiotherapy at a PSA level of less than 1 ng/mL. RTOG consensus CTVs that included both the prostate bed and the pelvic lymph nodes were contoured on the CT dataset of the PET/CT image by a radiation oncologist masked to the PET component. 68Ga-PSMA-11 PET/CT images were analyzed by a nuclear medicine physician. 68Ga-PSMA-11-positive lesions not covered by planning volumes based on the consensus CTVs were considered to have a potential major impact on treatment planning. Results: The median PSA level at the time of 68Ga-PSMA-11 PET/CT was 0.48 ng/mL (range, 0.03-1 ng/mL). One hundred thirty-two of 270 patients (49%) had a positive 68Ga-PSMA-11 PET/CT result. Fifty-two of 270 (19%) had at least one PSMA-11-positive lesion not covered by the consensus CTVs. Thirty-three of 270 (12%) had extrapelvic PSMA-11-positive lesions, and 19 of 270 (7%) had PSMA-11-positive lesions within the pelvis but not covered by the consensus CTVs. The 2 most common 68Ga-PSMA-11-positive lesion locations outside the consensus CTVs were bone (23/52, 44%) and perirectal lymph nodes (16/52, 31%). Conclusion: Post hoc analysis of 68Ga-PSMA-11 PET/CT implied a major impact on SRT planning in 52 of 270 patients (19%) with PCa early BCR (PSA < 1.0 ng/mL). This finding justifies a randomized imaging trial of SRT with or without 68Ga-PSMA-11 PET/CT investigating its potential benefit on clinical outcome.
Keywords: PET/CT; PSMA; prostate cancer; recurrence; salvage radiotherapy.
© 2018 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
Comment in
-
PSMA PET: Transformational Change in Prostate Cancer Management?J Nucl Med. 2018 Feb;59(2):228-229. doi: 10.2967/jnumed.117.203604. Epub 2017 Dec 14. J Nucl Med. 2018. PMID: 29242400 No abstract available.
Similar articles
-
68Ga-PSMA-11 PET/CT in prostate cancer patients with biochemical recurrence after radical prostatectomy and PSA <0.5 ng/ml. Efficacy and impact on treatment strategy.Eur J Nucl Med Mol Imaging. 2019 Jan;46(1):11-19. doi: 10.1007/s00259-018-4066-4. Epub 2018 Jun 15. Eur J Nucl Med Mol Imaging. 2019. PMID: 29905907
-
Potential Impact of 68Ga-PSMA-11 PET/CT on the Planning of Definitive Radiation Therapy for Prostate Cancer.J Nucl Med. 2018 Nov;59(11):1714-1721. doi: 10.2967/jnumed.118.209387. Epub 2018 Apr 13. J Nucl Med. 2018. PMID: 29653978 Free PMC article. Clinical Trial.
-
68Ga-PSMA-11 PET/CT in recurrent prostate cancer: efficacy in different clinical stages of PSA failure after radical therapy.Eur J Nucl Med Mol Imaging. 2019 Jan;46(1):31-39. doi: 10.1007/s00259-018-4189-7. Epub 2018 Oct 22. Eur J Nucl Med Mol Imaging. 2019. PMID: 30350010 Clinical Trial.
-
68Ga-Labeled Prostate-specific Membrane Antigen Ligand Positron Emission Tomography/Computed Tomography for Prostate Cancer: A Systematic Review and Meta-analysis.Eur Urol Focus. 2018 Sep;4(5):686-693. doi: 10.1016/j.euf.2016.11.002. Epub 2016 Nov 15. Eur Urol Focus. 2018. PMID: 28753806
-
Use of gallium-68 prostate-specific membrane antigen positron-emission tomography for detecting lymph node metastases in primary and recurrent prostate cancer and location of recurrence after radical prostatectomy: an overview of the current literature.BJU Int. 2020 Feb;125(2):206-214. doi: 10.1111/bju.14944. Epub 2019 Nov 29. BJU Int. 2020. PMID: 31680398 Free PMC article. Review.
Cited by
-
Phase 3 multicenter randomized trial of PSMA PET/CT prior to definitive radiation therapy for unfavorable intermediate-risk or high-risk prostate cancer [PSMA dRT]: study protocol.BMC Cancer. 2021 May 7;21(1):512. doi: 10.1186/s12885-021-08026-w. BMC Cancer. 2021. PMID: 33962579 Free PMC article.
-
Prognostic significance of a negative PSMA PET/CT in biochemical recurrence of prostate cancer.Cancer Imaging. 2024 Aug 30;24(1):117. doi: 10.1186/s40644-024-00752-1. Cancer Imaging. 2024. PMID: 39210431 Free PMC article.
-
Prospective comparison of 68Ga-PSMA PET/CT, 18F-sodium fluoride PET/CT and diffusion weighted-MRI at for the detection of bone metastases in biochemically recurrent prostate cancer.Eur J Nucl Med Mol Imaging. 2018 Oct;45(11):1884-1897. doi: 10.1007/s00259-018-4058-4. Epub 2018 Jun 6. Eur J Nucl Med Mol Imaging. 2018. PMID: 29876619
-
High Detection Rates for Prostate-specific Membrane Antigen-avid Prostate Cancer Recurrence at Low Prostate-specific Antigen levels on Extended Axial Field-of-view Positron Emission Tomography/Computed Tomography.Eur Urol Open Sci. 2024 Dec 7;71:49-56. doi: 10.1016/j.euros.2024.11.008. eCollection 2025 Jan. Eur Urol Open Sci. 2024. PMID: 39720335 Free PMC article.
-
Whole pelvis vs. hemi pelvis elective nodal radiotherapy in patients with PSMA-positive nodal recurrence after radical prostatectomy - a retrospective multi-institutional propensity score analysis.Eur J Nucl Med Mol Imaging. 2024 Oct;51(12):3770-3781. doi: 10.1007/s00259-024-06802-x. Epub 2024 Jun 28. Eur J Nucl Med Mol Imaging. 2024. PMID: 38940843 Free PMC article.
References
-
- Han M, Partin AW, Zahurak M, Piantadosi S, Epstein JI, Walsh PC. Biochemical (prostate specific antigen) recurrence probability following radical prostatectomy for clinically localized prostate cancer. J Urol. 2003;169:517–523. - PubMed
-
- Thompson IM, Valicenti RK, Albertsen P, et al. Adjuvant and salvage radiotherapy after prostatectomy: AUA/ASTRO guideline. J Urol. 2013;190:441–449. - PubMed
-
- King CR. Adjuvant versus salvage radiotherapy for high-risk prostate cancer patients. Semin Radiat Oncol. 2013;23:215–221. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous