

Airway surface liquid pH is not acidic in children with cystic fibrosis
- PMID: 29123085
- PMCID: PMC5680186
- DOI: 10.1038/s41467-017-00532-5
Airway surface liquid pH is not acidic in children with cystic fibrosis
Abstract
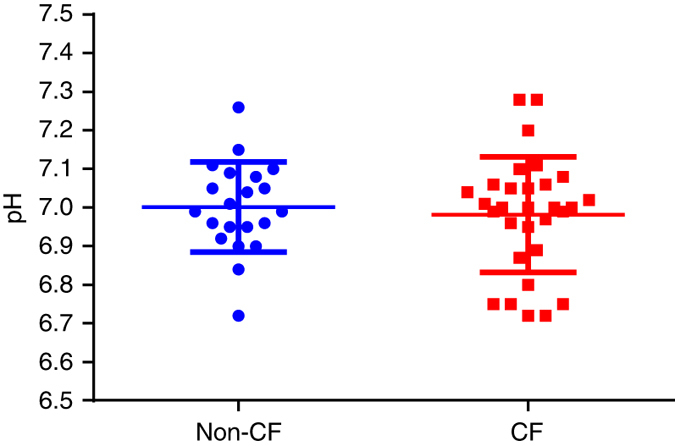
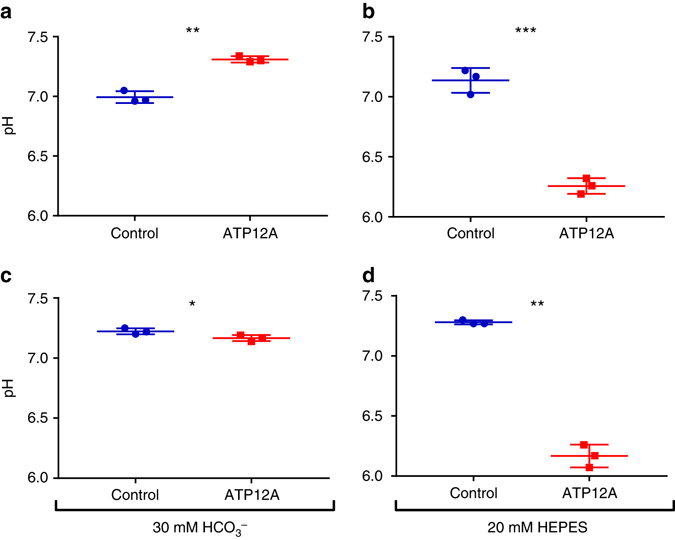
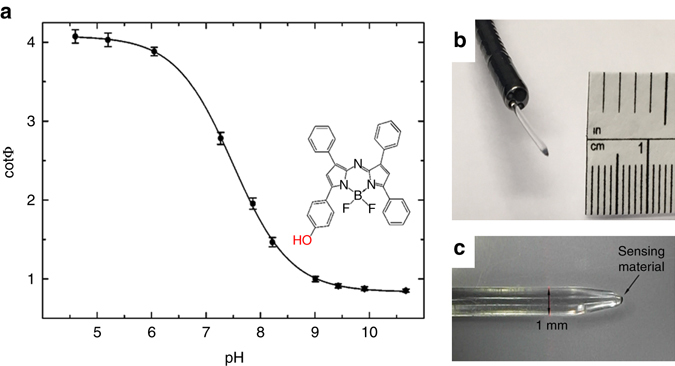
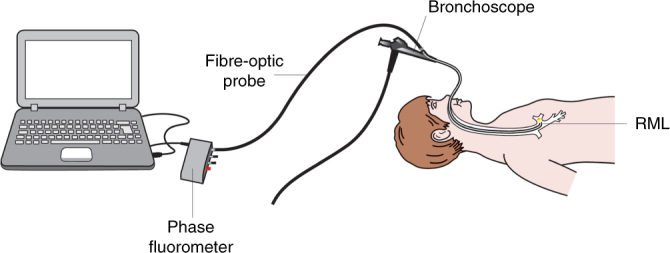
Modulation of airway surface liquid (ASL) pH has been proposed as a therapy for cystic fibrosis (CF). However, evidence that ASL pH is reduced in CF is limited and conflicting. The technical challenges associated with measuring ASL pH in vivo have precluded accurate measurements in humans. In order to address this deficiency, ASL pH was measured in vivo in children using a novel luminescent technology integrated with fibre-optic probes. Here we show that ASL pH in children with CF is similar to that of children without CF. Findings were supported by highly controlled direct pH measurements in primary human airway epithelial cell culture models, which also suggest that the potential ASL pH gradient produced by defective apical ion transport is balanced out by paracellular shunting of acid/base. Thus, reduced baseline ASL pH is unlikely to be an important pathobiological factor in early CF lung disease.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
References
-
- Cystic Fibrosis Foundation. https://www.cff.org. 2017.
-
- Cystic Fibrosis Canada. http://www.cysticfibrosis.ca/cf-care/cf-registry. 2017.
-
- Cystic Fibrosis Australia. http://www.cysticfibrosis.org.au. 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
