

Alveolar-capillary reserve during exercise in patients with chronic obstructive pulmonary disease
- PMID: 29123389
- PMCID: PMC5661445
- DOI: 10.2147/COPD.S142523
Alveolar-capillary reserve during exercise in patients with chronic obstructive pulmonary disease
Abstract
Background: Factors limiting exercise in patients with COPD are complex. With evidence for accelerated pulmonary vascular aging, destruction of alveolar-capillary bed, and hypoxic pulmonary vasoconstriction, the ability to functionally expand surface area during exercise may become a primary limitation.
Purpose: To quantify measures of alveolar-capillary recruitment during exercise and the relationship to exercise capacity in a cohort of COPD patients.
Methods: Thirty-two subjects gave consent (53% male, with mean ± standard deviation age 66±9 years, smoking 35±29 pack-years, and Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification of 0-4: 2.3±0.8), filled out the St George's Respiratory Questionnaire (SGRQ) to measure quality of life, had a complete blood count drawn, and underwent spirometry. The intrabreath (IB) technique for lung diffusing capacity for carbon monoxide (IBDLCO) and pulmonary blood flow (IBQc, at rest) was also performed. Subsequently, they completed a cycle ergometry test to exhaustion with measures of oxygen saturation and expired gases.
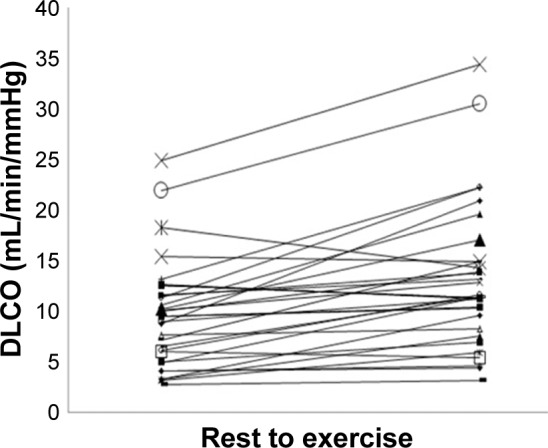
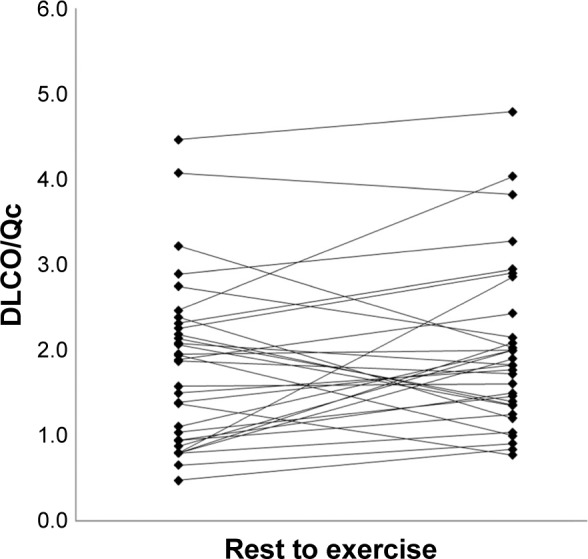
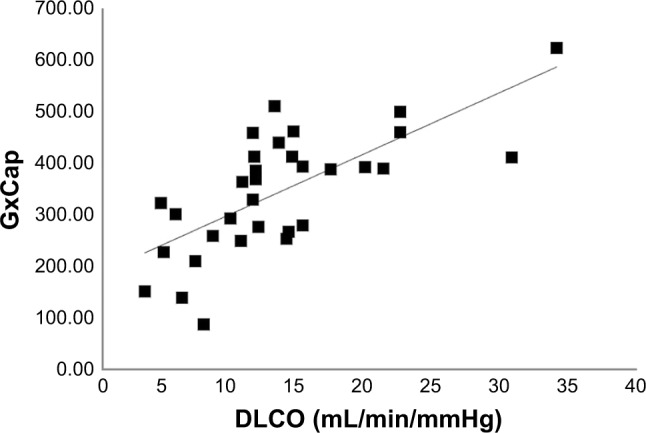
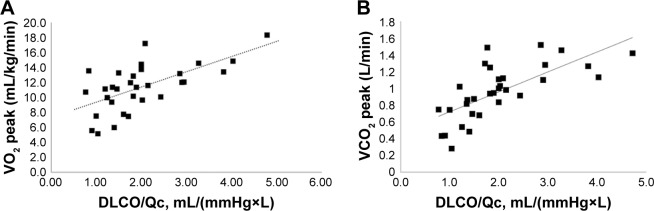
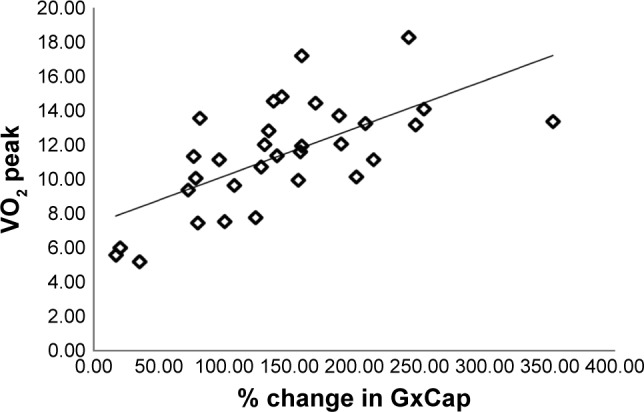
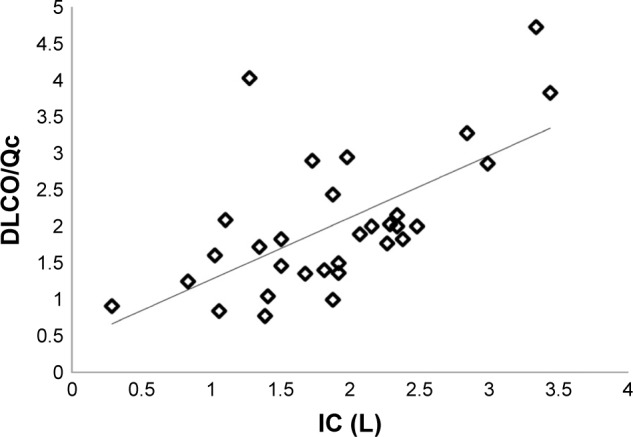
Results: Baseline average measures were 44±21 for SGRQ score and 58±11 for FEV1/FVC. Peak oxygen consumption (VO2) was 11.4±3.1 mL/kg/min (49% predicted). The mean resting IBDLCO was 9.7±5.4 mL/min/mmHg and IBQc was 4.7±0.9 L/min. At the first workload, heart rate (HR) increased to 92±11 bpm, VO2 was 8.3±1.4 mL/kg/min, and IBDLCO and IBQc increased by 46% and 43%, respectively, compared to resting values (p,0.01). The IBDLCO/Qc ratio averaged 2.0±1.1 at rest and remained constant during exercise with marked variation across subjects (range: 0.8-4.8). Ventilatory efficiency plateaued at 37±5 during exercise, partial pressure of mix expired CO2/partial pressure of end tidal CO2 ratio ranged from 0.63 to 0.67, while a noninvasive index of pulmonary capacitance, O2 pulse × PetCO2 (GxCap) rose to 138%. The exercise IBDLCO/Qc ratio was related to O2 pulse (VO2/HR, r=0.58, p<0.01), and subjects with the highest exercise IBDLCO/Qc ratio or the greatest rise from rest had the highest peak VO2 values (r=0.65 and 0.51, respectively, p<0.05). Of the noninvasive gas exchange measures of pulmonary vascular function, GxCap was most closely associated with DLCO, DLCO/Qc, and VO2 peak.
Conclusion: COPD patients who can expand gas exchange surface area as assessed with DLCO during exercise relative to pulmonary blood flow have a more preserved exercise capacity.
Keywords: COPD; airflow limitation; cardiopulmonary exercise testing; diffusion capacity; dyspnea; exercise intolerance; lung gas transfer.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Influence of resting lung diffusion on exercise capacity in patients with COPD.BMC Pulm Med. 2017 Aug 25;17(1):117. doi: 10.1186/s12890-017-0454-y. BMC Pulm Med. 2017. PMID: 28841877 Free PMC article.
-
Low resting diffusion capacity, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease.J Appl Physiol (1985). 2019 Oct 1;127(4):1107-1116. doi: 10.1152/japplphysiol.00341.2019. Epub 2019 Aug 1. J Appl Physiol (1985). 2019. PMID: 31369329
-
Influence of dietary nitrate supplementation on lung function and exercise gas exchange in COPD patients.Nitric Oxide. 2018 Jun 1;76:53-61. doi: 10.1016/j.niox.2018.03.009. Epub 2018 Mar 13. Nitric Oxide. 2018. PMID: 29549005 Clinical Trial.
-
Chronic obstructive pulmonary disease with mild airflow limitation: current knowledge and proposal for future research - a consensus document from six scientific societies.Int J Chron Obstruct Pulmon Dis. 2017 Aug 29;12:2593-2610. doi: 10.2147/COPD.S132236. eCollection 2017. Int J Chron Obstruct Pulmon Dis. 2017. PMID: 28919728 Free PMC article. Review.
-
Effects of Exercise Training on Cardiopulmonary Function and Quality of Life in Elderly Patients with Pulmonary Fibrosis: A Meta-Analysis.Int J Environ Res Public Health. 2021 Jul 18;18(14):7643. doi: 10.3390/ijerph18147643. Int J Environ Res Public Health. 2021. PMID: 34300094 Free PMC article. Review.
Cited by
-
Utility of Cardiopulmonary Exercise Testing in Chronic Obstructive Pulmonary Disease: A Review.Int J Chron Obstruct Pulmon Dis. 2023 Dec 5;18:2895-2910. doi: 10.2147/COPD.S432841. eCollection 2023. Int J Chron Obstruct Pulmon Dis. 2023. PMID: 38089541 Free PMC article. Review.
-
Lower DLco% identifies exercise pulmonary hypertension in patients with parenchymal lung disease referred for dyspnea.Pulm Circ. 2020 Feb 19;10(1):2045894019891912. doi: 10.1177/2045894019891912. eCollection 2020 Jan-Mar. Pulm Circ. 2020. PMID: 32128158 Free PMC article.
-
Pulmonary diffusing capacity for carbon monoxide and nitric oxide after COVID-19: A prospective cohort study (the SECURe study).Exp Physiol. 2024 May;109(5):652-661. doi: 10.1113/EP091757. Epub 2024 Mar 26. Exp Physiol. 2024. PMID: 38532277 Free PMC article.
-
Alveolar Air and O2 Uptake During Exercise in Patients With Heart Failure.J Card Fail. 2018 Oct;24(10):695-705. doi: 10.1016/j.cardfail.2018.08.001. Epub 2018 Aug 10. J Card Fail. 2018. PMID: 30103021 Free PMC article.
-
Exertional ventilation/carbon dioxide output relationship in COPD: from physiological mechanisms to clinical applications.Eur Respir Rev. 2021 Sep 15;30(161):200190. doi: 10.1183/16000617.0190-2020. Print 2021 Sep 30. Eur Respir Rev. 2021. PMID: 34526312 Free PMC article. Review.
References
-
- Dempsey JA. J.B. Wolffe memorial lecture. Is the lung built for exercise? Med Sci Sports Exerc. 1986;18(2):143–155. - PubMed
-
- Rampulla C, Marconi C, Beulcke G, Amaducci S. Correlations between lung-transfer factor, ventilation, and cardiac output during exercise. Respiration. 1976;33(6):405–415. - PubMed
-
- Montes de Oca M, Rassulo J, Celli BR. Respiratory muscle and cardiopulmonary function during exercise in very severe COPD. Am J Respir Crit Care Med. 1996;154(5):1284–1289. - PubMed
-
- Fujii T, Kurihara N, Fujimoto S, Hirata K, Yoshikawa J. Role of pulmonary vascular disorder in determining exercise capacity in patients with severe chronic obstructive pulmonary disease. Clin Physiol. 1996;16(5):521–533. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
