

Descending necrotizing mediastinitis: 5 years of published data in Japan
- PMID: 29123684
- PMCID: PMC5667189
- DOI: 10.1002/ams2.56
Descending necrotizing mediastinitis: 5 years of published data in Japan
Abstract
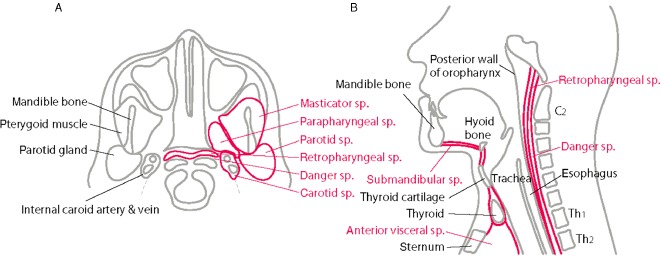
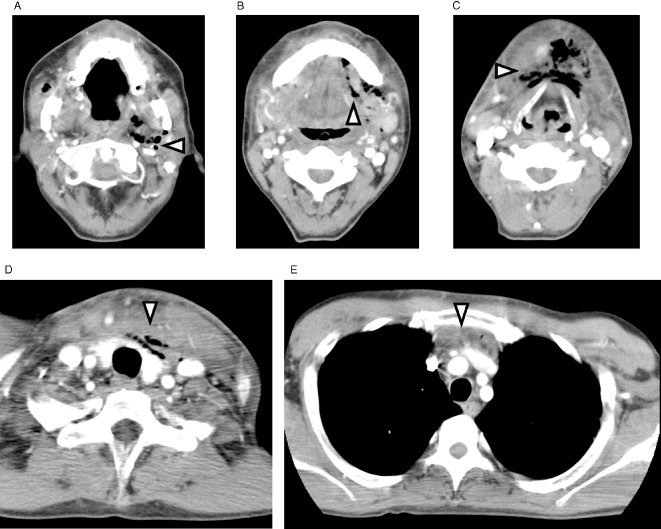
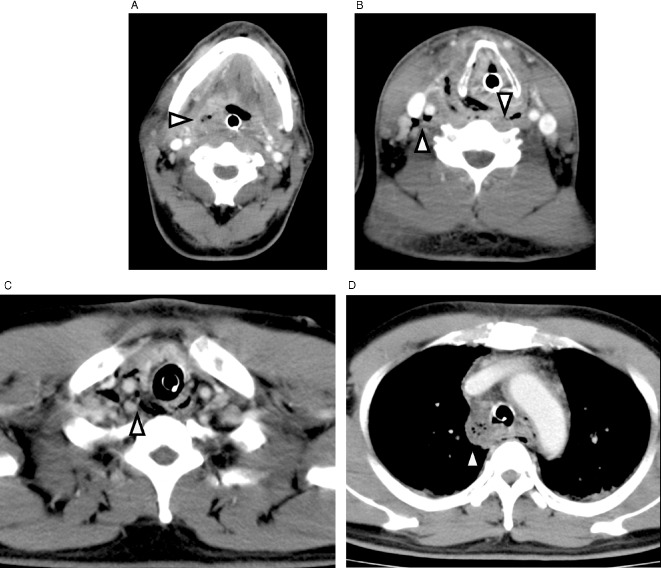
Descending necrotizing mediastinitis implies infection originating from the neck, most commonly an oropharyngeal or odontogenic focus, that spreads in the cervical fascial spaces and descends into the mediastinum. Early diagnosis is essential because descending necrotizing mediastinitis can rapidly progress to septic shock and organ failure. A comprehensive review of the current data of descending necrotizing mediastinitis in Japan was carried out using PubMed and ICHUSHI from the last 5 years. The symptoms, origins, comorbid conditions, treatment modalities, complications, and survival rates were analyzed. Tonsillar and pharyngeal origin was more identified compared to odontogenic origin. More than one-third of patients were diabetic and 28% of them were not identified as having any comorbidity. Streptococcus sp. and anaerobes were most isolated, reflecting the microflora of the oral cavity. Of the broad antibiotics, carbapenem was the most used as treatment, and clindamycin was the most co-given. Mediastinal drainage approach varied widely and the optimal approach is controversial. Twenty-one patients were treated with video-assisted thoracic surgical drainage and 15 cases by percutaneous catheter drainage, whereas transcervical approach was applied in 25 patients and thoracotomy was carried out in 21 patients. The overall mortality was 5.6%. Many authors advocated that the most effective management tool is a high degree of clinical suspicion followed by prompt and adequate drainage with intensive care including hemodynamic and nutritional support and repeat computer tomographic monitoring.
Keywords: Airway emergency; cervical necrotizing fasciitis; descending necrotizing mediastinitis; percutaneous catheter drainage; video‐assisted thoracoscopic drainage.
Figures
Similar articles
-
Descending necrotizing mediastinitis: transcervical drainage is not enough.Ann Thorac Surg. 1990 May;49(5):780-4. doi: 10.1016/0003-4975(90)90022-x. Ann Thorac Surg. 1990. PMID: 2288561 Review.
-
Thoracoscopic management of descending necrotizing mediastinitis.Chest. 1997 Sep;112(3):850-4. doi: 10.1378/chest.112.3.850. Chest. 1997. PMID: 9315828
-
Descending necrotizing mediastinitis. Advantage of mediastinal drainage with thoracotomy.J Thorac Cardiovasc Surg. 1994 Jan;107(1):55-61. J Thorac Cardiovasc Surg. 1994. PMID: 8283919
-
Guideline of surgical management based on diffusion of descending necrotizing mediastinitis.Jpn J Thorac Cardiovasc Surg. 1999 Jan;47(1):14-9. doi: 10.1007/BF03217934. Jpn J Thorac Cardiovasc Surg. 1999. PMID: 10077888
-
Cervical necrotizing fasciitis with descending mediastinitis: literature review and case report.J Oral Maxillofac Surg. 2012 Jun;70(6):1342-50. doi: 10.1016/j.joms.2011.05.007. Epub 2011 Aug 6. J Oral Maxillofac Surg. 2012. PMID: 21820786 Review.
Cited by
-
Demographic, clinical, and paraclinical features of patients operated with the diagnosis of acute descending necrotizing mediastinitis: a retrospective study in Southern Iran.J Cardiothorac Surg. 2023 Dec 8;18(1):354. doi: 10.1186/s13019-023-02416-w. J Cardiothorac Surg. 2023. PMID: 38066576 Free PMC article.
-
Distribution of descending necrotizing mediastinitis and efficacy of distribution-specific drainage.J Thorac Dis. 2020 May;12(5):2380-2387. doi: 10.21037/jtd.2020.03.82. J Thorac Dis. 2020. PMID: 32642143 Free PMC article.
-
The efficacy of thoracoscopic surgery for descending necrotizing mediastinitis.Interdiscip Cardiovasc Thorac Surg. 2023 Apr 3;36(4):ivad053. doi: 10.1093/icvts/ivad053. Interdiscip Cardiovasc Thorac Surg. 2023. PMID: 37018143 Free PMC article.
-
Descending necrotising mediastinitis: a rare entity in children.BMJ Case Rep. 2024 Mar 7;17(3):e258304. doi: 10.1136/bcr-2023-258304. BMJ Case Rep. 2024. PMID: 38453221
-
Descending necrotizing mediastinitis complicating deep neck abscesses: clinical features and prognostic assessment in 45 ICU patients.Eur Arch Otorhinolaryngol. 2025 May;282(5):2617-2625. doi: 10.1007/s00405-024-09179-7. Epub 2024 Dec 23. Eur Arch Otorhinolaryngol. 2025. PMID: 39714619
References
-
- Estrera AS, Landay MJ, Grisham JM, Sinn DP, Platt MR. Descending necrotizing mediastinitis. Surg. Gynecol. Obstet. 1983; 157: 545–552. - PubMed
-
- Sarna T, Sengupta T, Miloro M, Kolokythas A. Cervical necrotizing fasciitis with descending mediastinitis: literature review and case report. J. Oral Maxillofac. Surg. 2012; 70: 1342–1350. - PubMed
-
- Son HS, Cho JH, Park SM, Sun K, Kim KT, Lee SH. Management of descending necrotizing mediastinitis using minimally invasive video‐assisted thoracoscopic surgery. Surg. Laparosc. Endosc. Percutan. Tech. 2006; 16: 379–382. - PubMed
-
- Ohno K, Yamasaki Y, Hatanaka N, Yamamoto S, Naitoh H, Kuwata K. [Mediastinoscopic drainage for descending necrotizing mediastinitis]. Jpn J. Thorac. Cardiovasc. Surg. 1998; 46: 175–178. (In Japanese.) - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
