

Relationship between systolic blood pressures measured in emergency department and outcomes in patients with subarachnoid hemorrhage
- PMID: 29123688
- PMCID: PMC5667197
- DOI: 10.1002/ams2.63
Relationship between systolic blood pressures measured in emergency department and outcomes in patients with subarachnoid hemorrhage
Abstract
Aim: High blood pressure is observed frequently in patients with subarachnoid hemorrhage who present to the emergency department. Although extremely high blood pressure is known to predict poor outcomes in patients with spontaneous intracerebral hemorrhage, the relationship between high blood pressure and outcomes has been studied less frequently in patients with subarachnoid hemorrhage.
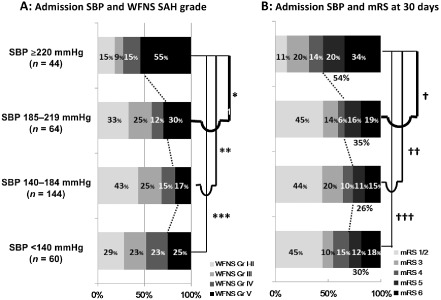
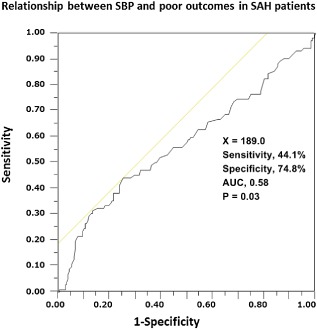
Methods: A retrospective study was carried out to evaluate whether high blood pressure observed in the emergency department was predictive of poor outcomes in patients with subarachnoid hemorrhage. Three-hundred and twelve subarachnoid hemorrhage patients who were admitted to our institution were quadrichotomized based on their initial systolic blood pressure: <140 mmHg (n = 60), 140-184 mmHg (n = 144), 185-219 mmHg (n = 64), and ≥220 mmHg (n = 44). Demographics including subarachnoid hemorrhage severity (World Federation of Neurosurgical Societies grade) and outcome variables evaluated with the modified Rankin scale 30 days after admission were compared among the four blood pressure groups. Furthermore, an effort was made to delineate a threshold value of systolic blood pressure predictive of outcomes by receiver operating characteristic curve analysis.
Results: The frequency of grade V subarachnoid hemorrhage in the ≥220 mmHg group (55%) was significantly higher than in the other three blood pressure groups. The frequency of patients scoring 5-6 on the modified Rankin scale in the ≥220 mmHg group (54%) was significantly higher than in the other three blood pressure groups. The cut-off systolic blood pressure value predicting poor outcomes (modified Rankin scale 5-6) determined by receiver operating characteristic curve analysis was 189 mmHg.
Conclusions: The higher proportion of grade V patients may be responsible for the worse outcomes in the group with systolic blood pressure ≥220 mmHg. Initial systolic blood pressure ≥220 mmHg may be a crude indicator of poor outcomes in patients with subarachnoid hemorrhage.
Keywords: Emergency department; high blood pressure; outcomes; predictability; subarachnoid hemorrhage.
Figures
References
-
- Inamasu J, Ito K, Sugimoto K, Watanabe E, Kato Y, Hirose Y. Cardiac wall motion abnormality associated with spontaneous intracerebral hemorrhage. Int. J. Cardiol. 2013; 168: 1667–1669. - PubMed
-
- Dandapani BK, Suzuki S, Kelley RE, Reyes‐Iglesias Y, Duncan RC. Relation between blood pressure and outcome in intracerebral hemorrhage. Stroke 1995; 26: 21–24. - PubMed
-
- Fogelholm R, Avikainen S, Murros K. Prognostic value and determinants of first‐day mean arterial pressure in spontaneous supratentorial intracerebral hemorrhage. Stroke 1997; 28: 1396–1400. - PubMed
-
- Okumura K, Ohya Y, Maehara A, Wakugami K, Iseki K, Takishita S. Effects of blood pressure levels on case fatality after acute stroke. J. Hypertens. 2005; 23: 1055–1060. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
