

Reduction of unexpected serious adverse events after introducing medical emergency team
- PMID: 29123731
- PMCID: PMC5649287
- DOI: 10.1002/ams2.101
Reduction of unexpected serious adverse events after introducing medical emergency team
Abstract
Aim: To assess the clinical benefits of introducing a medical emergency team system for early medical intervention in hospital care.
Methods: This prospective analysis included all cases of medical emergency team activation during the first year after the introduction of the medical emergency team system at Chiba University Hospital (Chiba, Japan) in February 2011. The rates of in-hospital mortality and unexpected events before and after introduction of the medical emergency team system were compared.
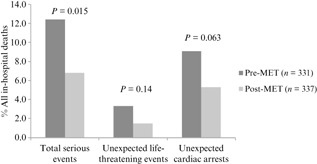
Results: The total number of medical emergency team activation calls was 83 (4.9 per 1,000 admissions). The activation of the medical emergency team system was requested most frequently from the general ward (56.6%) and by a physician (57.8%), with the most important reasons for activation being cardiac arrest (37.3%), breathing abnormality (33.7%), and impaired consciousness (32.5%). The most frequent medical interventions by the medical emergency team were intubation (43.3%) and oxygen inhalation (41.0%). Approximately one-half of the patients requiring activation of the medical emergency team system were critically ill and needed subsequent intensive care unit admission. Although no significant difference was observed between the pre- and post- medical emergency team in-hospital mortalities (2.1% versus 2.0%, respectively), the incidence rate of serious events significantly decreased (12.4% versus 6.8%, respectively; P = 0.015).
Conclusion: Most patients requiring activation of the medical emergency team system were critically ill and needed emergency treatment at the location of the medical emergency team activation, with subsequent critical care. Although the introduction of the medical emergency team system did not affect the in-hospital mortality rate, it reduced the incidence of unexpected serious adverse events, suggesting that it may be clinically useful.
Keywords: Medical emergency team; other; rapid response system.
Figures
References
-
- Wissenberg M, Lippert FK, Folke F et al Association of national initiatives to improve cardiac arrest management with rates of bystander intervention and patient survival after out‐of‐hospital cardiac arrest. JAMA 2013; 310: 1377–1384. - PubMed
-
- Schein RM, Hazday N, Pena M, Ruben BH, Sprung CL. Clinical antecedents to in‐hospital cardiopulmonary arrest. Chest 1990; 98: 1388–1392. - PubMed
-
- Hodgetts TJ, Kenward G, Vlachonikolis IG, Payne S, Castle N. The identification of risk factors for cardiac arrest and formulation of activation criteria to alert a medical emergency team. Resuscitation 2002; 54: 125–131. - PubMed
-
- Jones DA, DeVita MA, Bellomo R. Rapid‐response teams. N. Engl. J. Med. 2011; 365: 139–146. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
