

Continuous veno-venous hemodialysis and filtration for extensive burn with severe hypernatremia
- PMID: 29123794
- PMCID: PMC5667236
- DOI: 10.1002/ams2.170
Continuous veno-venous hemodialysis and filtration for extensive burn with severe hypernatremia
Abstract
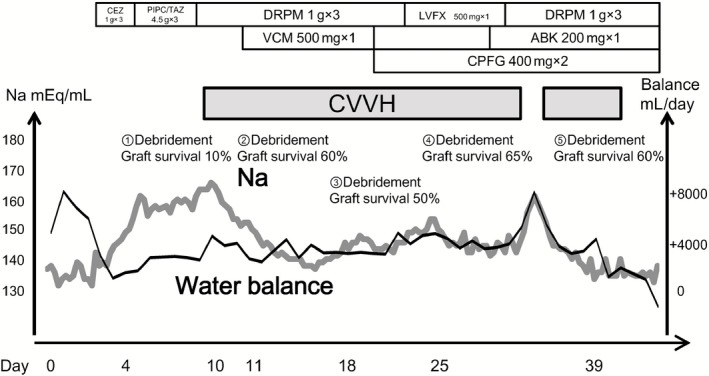
Case: A 51-year-old man presented with severe burns, with a burn index of 33.5. Relaxation incisions were made in the trunk and right arm. Ringer's solution (12,000 mL) was used as initial fluid therapy for the first 24 h. The patient's serum Na level gradually increased to 170 mEq/L; infusion was carried out to correct the hypernatremia. Continuous veno-venous hemodialysis and filtration succeeded in maintaining the serum Na level at approximately 145 mEq/L.
Outcome: After the initiation of continuous veno-venous hemodialysis and filtration, the skin graft survival rate improved markedly with the normalization of the Na level, and the patient recovered smoothly. He was discharged on foot.
Conclusion: Hypernatremia, frequently observed in patients with extensive burns, is considered to be markedly disadvantageous for the survival of skin grafts. Continuous veno-venous hemodialysis and filtration may be one of the options for the treatment of refractory hypernatremia in severe burns.
Keywords: Burn; continuous veno‐venous hemodialysis and filtration; hypernatremia; renal replacement therapy; skin graft.
Figures


Similar articles
-
Continuous veno-venous hemofiltration in the treatment of severely burned patients with acute hypernatremia: A retrospective study of 13 cases.Int J Artif Organs. 2020 Jun;43(6):416-421. doi: 10.1177/0391398819893381. Epub 2019 Dec 18. Int J Artif Organs. 2020. PMID: 31849258
-
[Successful treatment of extreme hypernatremia by continuous veno-venous hemodiafiltration].Nephrol Ther. 2015 Nov;11(6):492-5. doi: 10.1016/j.nephro.2015.04.004. Epub 2015 Jul 11. Nephrol Ther. 2015. PMID: 26169976 French.
-
Veno-venous continuous renal replacement therapy for burned patients with acute renal failure.Burns. 2000 Nov;26(7):638-43. doi: 10.1016/s0305-4179(00)00010-3. Burns. 2000. PMID: 10925188
-
Therapeutic hypernatremia management during continuous renal replacement therapy with elevated intracranial pressures and respiratory failure.Rev Endocr Metab Disord. 2019 Mar;20(1):65-75. doi: 10.1007/s11154-019-09483-2. Rev Endocr Metab Disord. 2019. PMID: 30848433 Review.
-
Fatal hypernatremia from exogenous salt intake: report of a case and review of the literature.Mayo Clin Proc. 1990 Dec;65(12):1587-94. doi: 10.1016/s0025-6196(12)62194-6. Mayo Clin Proc. 1990. PMID: 2255221 Review.
References
-
- Ebrahim MK, George A, Bang RL. Only some septicaemic patients develop hypernatremia in the burn intensive care unit: Why? Burns 2002; 28: 543–547. - PubMed
-
- Baxter CR. Fluid volume and electrolyte changes of the early postburn period. Clin. Plast. Surg. 1974; 1: 693–703. - PubMed
-
- Lin M, Liu SJ, Lim IT. Disorders of water imbalance. Emerg. Med. Clin. North Am. 2005; 23: 749–770, ix. - PubMed
-
- Archer SB, Henke A, Greenhalgh DG, Warden GD. The use of sheet autografts to cover extensive burns in patients. J. Burn Care Rehabil. 1998; 19 (1 Pt 1): 33–38. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
