

Cardiocerebral and cardiopulmonary resuscitation - 2017 update
- PMID: 29123868
- PMCID: PMC5674458
- DOI: 10.1002/ams2.281
Cardiocerebral and cardiopulmonary resuscitation - 2017 update
Abstract
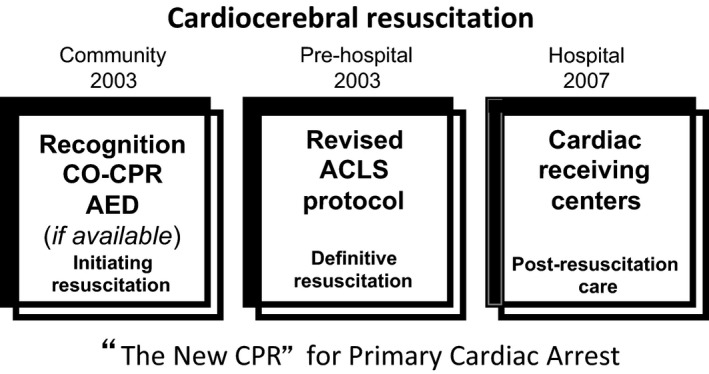
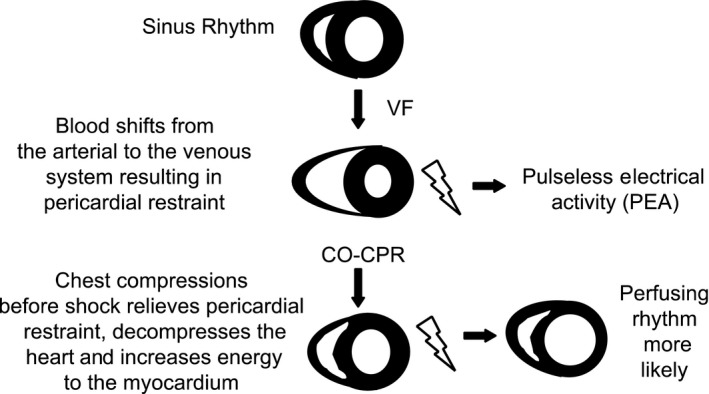
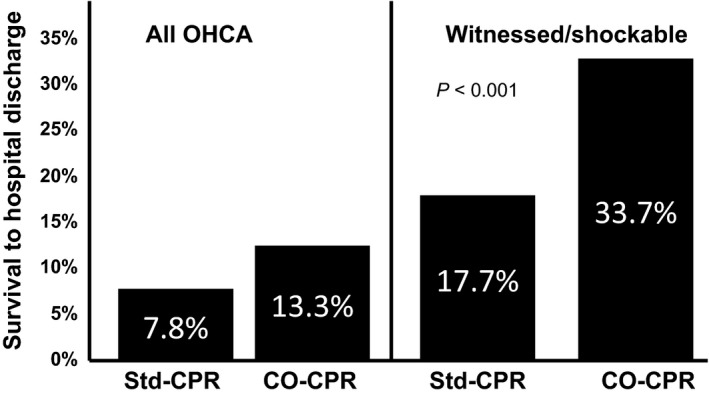
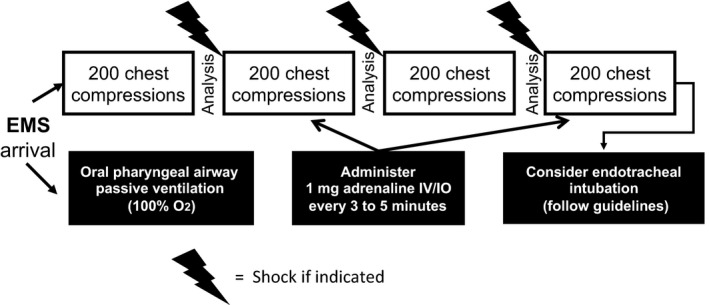
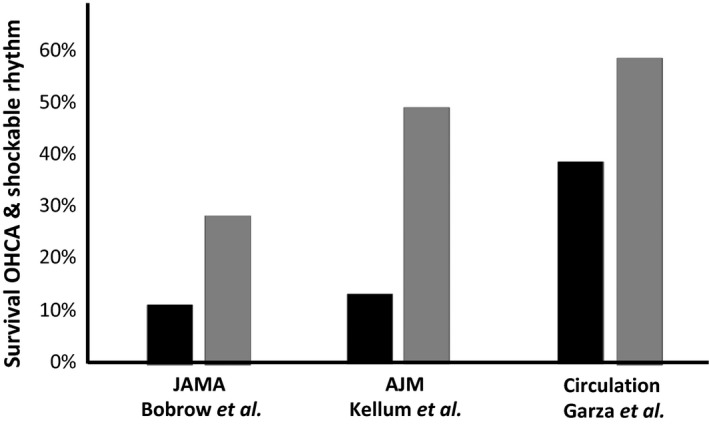
Sudden cardiac arrest is a major public health problem in the industrialized nations of the world. Yet, in spite of recurrent updates of the guidelines for cardiopulmonary resuscitation and emergency cardiac care, many areas have suboptimal survival rates. Cardiocerebral resuscitation, a non-guidelines approach to therapy of primary cardiac arrest based on our animal research, was instituted in Tucson (AZ, USA) in 2002 and subsequently adopted in other areas of the USA. Survival rates of patients with primary cardiac arrest and a shockable rhythm significantly improved wherever it was adopted. Cardiocerebral resuscitation has three components: the community, the pre-hospital, and the hospital. The community component emphasizes bystander recognition and chest compression only resuscitation. Its pre-hospital or emergency medical services component emphasizes: (i) urgent initiation of 200 uninterrupted chest compressions before and after each indicated single defibrillation shock, (ii) delayed endotracheal intubation in favor of passive delivery of oxygen by a non-rebreather mask, (iii) early adrenaline administration. The hospital component was added later. The national and international guidelines for cardiopulmonary resuscitation and emergency medical services are still not optimal, for several reasons, including the fact that they continue to recommend the same approach for two entirely different etiologies of cardiac arrest: primary cardiac arrest, often caused by ventricular fibrillation, where the arterial blood oxygenation is little changed at the time of the arrest, and secondary cardiac arrest from severe respiratory insufficiency, where the arterial blood is severely desaturated at the time of cardiac arrest. These different etiologies need different approaches to therapy.
Keywords: Bystander CPR; out‐of‐hospital cardiac arrest; primary cardiac arrest; respiratory arrest.
Figures
Similar articles
-
Cardiocerebral Resuscitation: An Approach to Improving Survival of Patients With Primary Cardiac Arrest.J Intensive Care Med. 2016 Jan;31(1):24-33. doi: 10.1177/0885066614544450. Epub 2014 Jul 30. J Intensive Care Med. 2016. PMID: 25077491 Review.
-
Cardiocerebral resuscitation improves survival of patients with out-of-hospital cardiac arrest.Am J Med. 2006 Apr;119(4):335-40. doi: 10.1016/j.amjmed.2005.11.014. Am J Med. 2006. PMID: 16564776
-
The cardiocerebral resuscitation protocol for treatment of out-of-hospital primary cardiac arrest.Scand J Trauma Resusc Emerg Med. 2012 Sep 15;20:65. doi: 10.1186/1757-7241-20-65. Scand J Trauma Resusc Emerg Med. 2012. PMID: 22980487 Free PMC article. Review.
-
2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: pediatric basic life support.Pediatrics. 2006 May;117(5):e989-1004. doi: 10.1542/peds.2006-0219. Pediatrics. 2006. PMID: 16651298
-
Cardiocerebral resuscitation for cardiac arrest.Am J Med. 2006 Jan;119(1):6-9. doi: 10.1016/j.amjmed.2005.06.067. Am J Med. 2006. PMID: 16431175 Review.
Cited by
-
Management of Cardiovascular Disease Patients with Periodontitis Requiring Dental Treatment - A KAP Study among Dental Students.J Pharm Bioallied Sci. 2024 Jul;16(Suppl 3):S2467-S2469. doi: 10.4103/jpbs.jpbs_352_24. Epub 2024 Jul 31. J Pharm Bioallied Sci. 2024. PMID: 39346245 Free PMC article.
-
Knowledge, Attitude, and Perceived Confidence in the Management of Medical Emergencies in the Dental Office: A Survey among the Dental Students and Interns.J Int Soc Prev Community Dent. 2017 Nov-Dec;7(6):364-369. doi: 10.4103/jispcd.JISPCD_414_17. Epub 2017 Dec 29. J Int Soc Prev Community Dent. 2017. PMID: 29387622 Free PMC article.
-
Hands-On Times, Adherence to Recommendations and Variance in Execution among Three Different CPR Algorithms: A Prospective Randomized Single-Blind Simulator-Based Trial.Int J Environ Res Public Health. 2020 Oct 29;17(21):7946. doi: 10.3390/ijerph17217946. Int J Environ Res Public Health. 2020. PMID: 33138109 Free PMC article. Clinical Trial.
-
Impact on awareness and knowledge of resuscitation by structured training of compression-only life support (COLS) among non-medical staff.Indian J Anaesth. 2023 Feb;67(Suppl 1):S48-S52. doi: 10.4103/ija.ija_324_22. Epub 2023 Feb 10. Indian J Anaesth. 2023. PMID: 37065940 Free PMC article.
-
Health-Care Providers' Knowledge, Attitudes, and Practices Regarding Adult Cardiopulmonary Resuscitation at Debre Markos Referral Hospital, Gojjam, Northwest Ethiopia.Adv Med Educ Pract. 2021 Jun 14;12:647-654. doi: 10.2147/AMEP.S293648. eCollection 2021. Adv Med Educ Pract. 2021. PMID: 34163280 Free PMC article.
References
-
- Roger VL, Go AS, Lloyd‐Jones DM. Executive summary: heart disease and stroke statistics‐2012 update: a report from the American Heart Association. Circulation 2012; 125: 188–97. - PubMed
-
- Lloyd‐Jones DM. Cardiovascular risk prediction: basic concepts, current status, and future directions. Circulation 2010; 121: 1768–77. - PubMed
-
- Spaulding SM, Joly L‐M, Rosenberg A et al Immediate coronary angiography in survivors of out‐of‐hospital cardiac arrest. N. Engl. J. Med. 1997; 336: 1629–33. - PubMed
-
- Ewy GA. Chest compression only cardiopulmonary resuscitation for primary cardiac arrest. Circulation 2016; 134: 695–697. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
