

Early administration of fibrinogen concentrates improves the short-term outcomes of severe pelvic fracture patients
- PMID: 29123874
- PMCID: PMC5674452
- DOI: 10.1002/ams2.268
Early administration of fibrinogen concentrates improves the short-term outcomes of severe pelvic fracture patients
Abstract
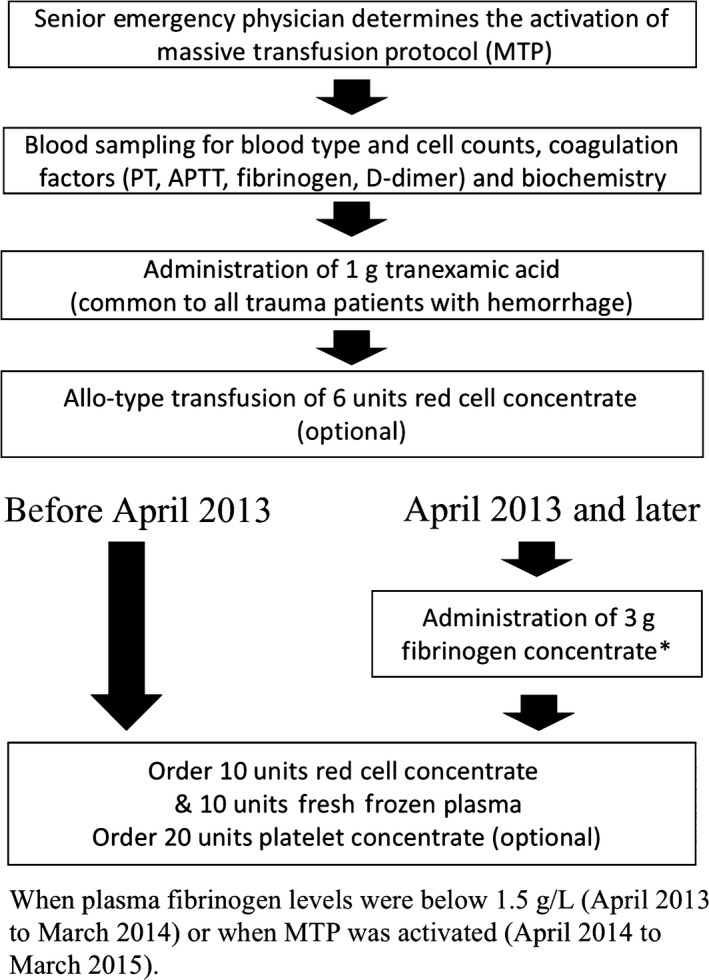
Aim: Hemorrhage from pelvic fracture is a major cause of mortality after blunt trauma. Several studies have suggested that early fibrinogen supplementation improves outcomes of traumatic hemorrhage. Thus, we revised our massive transfusion protocol (MTP) in April 2013 to include early off-label administration of fibrinogen concentrate. The objective of this study was to evaluate the impact of the revision on the short-term outcomes of pelvic fracture patients.
Methods: This was a single-center, retrospective, cohort study. A total of 224 consecutive pelvic fracture patients hospitalized in Saitama Medical Center (Saitama, Japan), 115 before the revision (Group E) and 109 after (Group L), were enrolled. Characteristics of the patients were compared between the groups. Impacts of the revision were evaluated by hazard ratios adjusted for characteristics, injury severity, and coagulation status using Cox's multivariate proportional hazard model. The impact was also evaluated by log-rank test and relative risk of 28-day mortality between the groups.
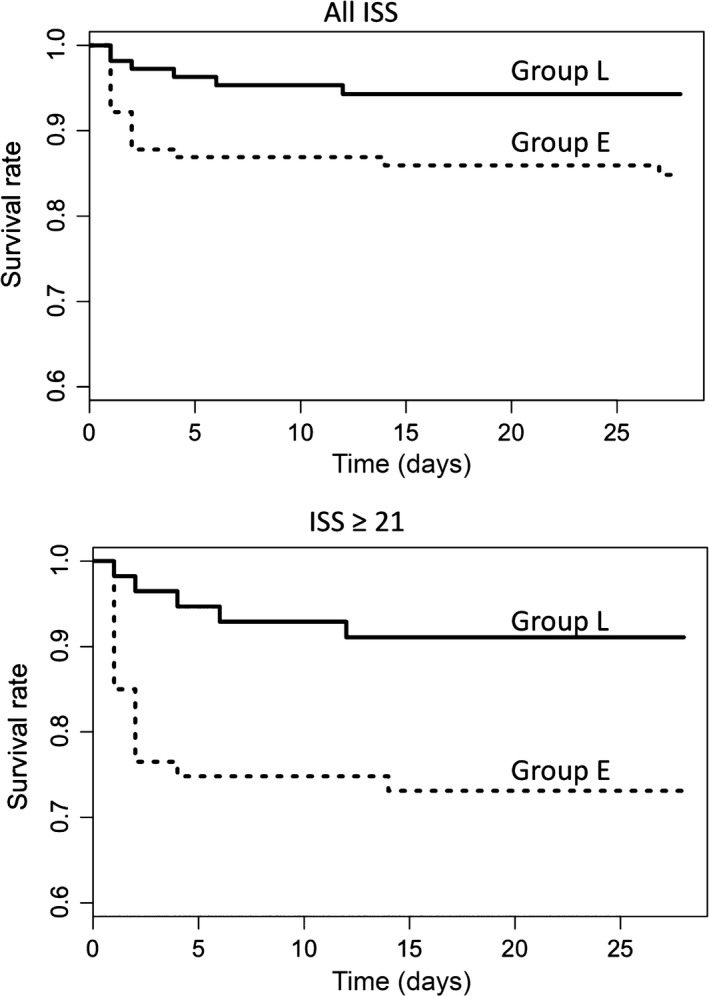
Results: The characteristics were equivalent between the groups. The multivariate analysis revealed that the revision of MTP was significantly related to improved survival with an adjusted hazard ratio (95% confidence interval) of 0.45 (0.07-0.97). The log-rank test gave χ2-test values of 5.2 (P = 0.022) and 6.7 (P = 0.009), and the relative risks were 0.37 (0.15-0.91) and 0.33 (0.13-0.84), in patients with all Injury Severity Scores and Injury Severity Score ≥21, respectively.
Conclusion: The revision of MTP to include aggressive off-label treatment with fibrinogen concentrate was related to improved short-term outcomes of severe pelvic fracture patients. However, due to the limitations of the study, the improvement could not be attributed totally to the revision.
Keywords: Blood coagulation disorders; fibrinogen; hemorrhage; pelvic bones; trauma.
Figures
Similar articles
-
Impact of initial coagulation and fibrinolytic markers on mortality in patients with severe blunt trauma: a multicentre retrospective observational study.Scand J Trauma Resusc Emerg Med. 2019 Feb 28;27(1):25. doi: 10.1186/s13049-019-0606-6. Scand J Trauma Resusc Emerg Med. 2019. PMID: 30819212 Free PMC article.
-
Bleeding Pelvic Fracture Patients: Evolution of Resuscitation Protocols.Scand J Surg. 2017 Sep;106(3):255-260. doi: 10.1177/1457496916683092. Epub 2017 Mar 1. Scand J Surg. 2017. PMID: 28737073
-
Early coagulation support protocol: A valid approach in real-life management of major trauma patients. Results from two Italian centres.Injury. 2019 Oct;50(10):1671-1677. doi: 10.1016/j.injury.2019.09.032. Injury. 2019. PMID: 31690405
-
[Hemoglobin-oriented and coagulation factor-based algorithm : Effect on transfusion needs and standardized mortality rate in massively transfused trauma patients].Anaesthesist. 2015 Nov;64(11):828-38. doi: 10.1007/s00101-015-0093-8. Epub 2015 Oct 9. Anaesthesist. 2015. PMID: 26453580 Review. German.
-
Massive transfusion protocols in nontrauma patients: A systematic review and meta-analysis.J Trauma Acute Care Surg. 2019 Mar;86(3):493-504. doi: 10.1097/TA.0000000000002101. J Trauma Acute Care Surg. 2019. PMID: 30376535
Cited by
-
Effects of in-house cryoprecipitate on transfusion usage and mortality in patients with multiple trauma with severe traumatic brain injury: a retrospective cohort study.Blood Transfus. 2020 Jan;18(1):6-12. doi: 10.2450/2019.0198-18. Epub 2019 Jan 22. Blood Transfus. 2020. PMID: 30747700 Free PMC article.
-
Medical equipment that improve safety and outcomes of inter-facility transportation of critically ill patients: A systematic review.Medicine (Baltimore). 2023 Jun 2;102(22):e33865. doi: 10.1097/MD.0000000000033865. Medicine (Baltimore). 2023. PMID: 37266640 Free PMC article.
-
Effect of early administration of fibrinogen replacement therapy in traumatic haemorrhage: a systematic review and meta-analysis of randomised controlled trials with narrative synthesis of observational studies.Crit Care. 2025 Jan 28;29(1):49. doi: 10.1186/s13054-025-05269-y. Crit Care. 2025. PMID: 39875966 Free PMC article.
-
Blood failure: traumatic hemorrhage and the interconnections between oxygen debt, endotheliopathy, and coagulopathy.Clin Exp Emerg Med. 2024 Mar;11(1):9-21. doi: 10.15441/ceem.23.127. Epub 2024 Mar 21. Clin Exp Emerg Med. 2024. PMID: 38018069 Free PMC article.
References
-
- Cullinane DC, Schiller HJ, Zielinski MD et al Eastern Association for the Surgery of Trauma practice management guidelines for hemorrhage in pelvic fracture – update and systematic review. J. Trauma 2011; 71: 1850–68. - PubMed
-
- Heetveld MJ, Harris I, Schlaphoff G, Balogh Z, D'Amours SK, Sugrue M. Hemodynamically unstable pelvic fractures: recent care and new guidelines. World J. Surg. 2004; 28: 904–9. - PubMed
-
- Khan S, Davenport R, Raza I et al Damage control resuscitation using blood component therapy in standard doses has a limited effect on coagulopathy during trauma hemorrhage. Intensive Care Med. 2015; 41: 239–47. - PubMed
-
- Hiippala ST, Myllyla GJ, Vahtera EM. Hemostatic factors and replacement of major blood loss with plasma‐poor Red Cell Concentrates. Anesth. Analg. 1995; 81: 360–5. - PubMed
-
- Scalea TM, Bochicchio KM, Lumpkins K et al Early aggressive use of fresh frozen plasma does not improve outcome in critically injured trauma patients. Ann. Surg. 2008; 248: 578–84. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
