

Mutations in JAK2 and Calreticulin genes are associated with specific alterations of the immune system in myelofibrosis
- PMID: 29123956
- PMCID: PMC5665081
- DOI: 10.1080/2162402X.2017.1345402
Mutations in JAK2 and Calreticulin genes are associated with specific alterations of the immune system in myelofibrosis
Abstract
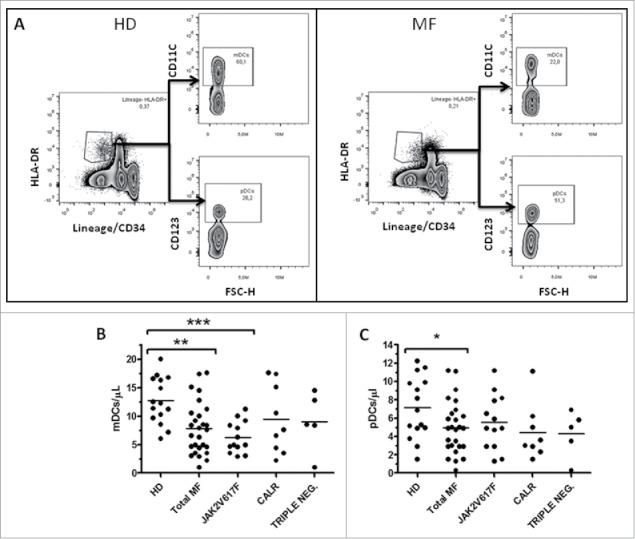
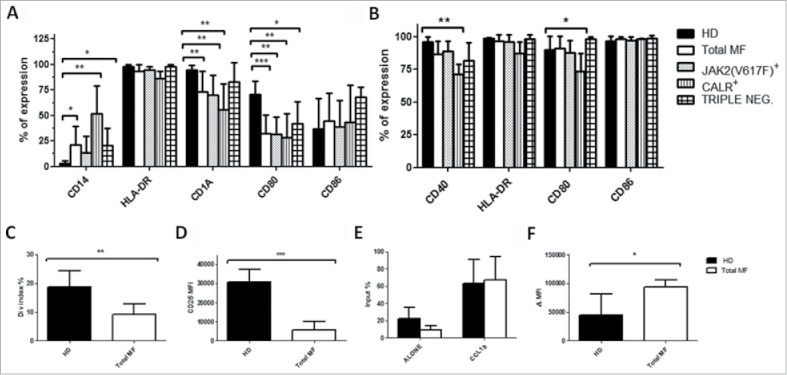
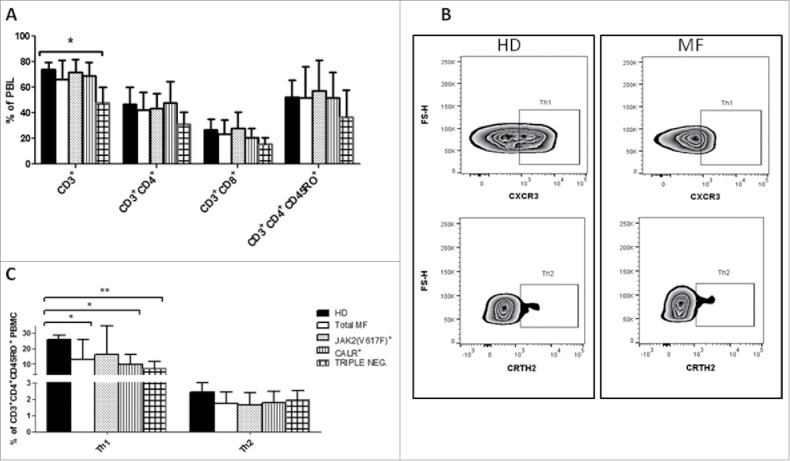
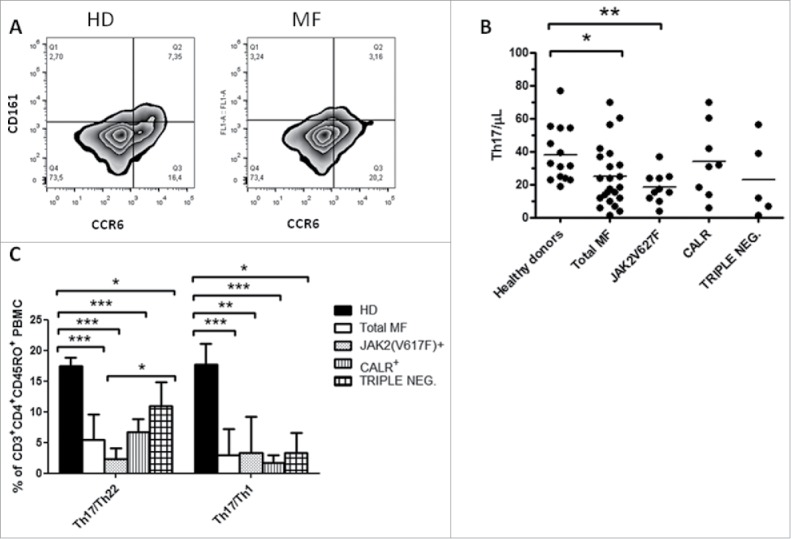
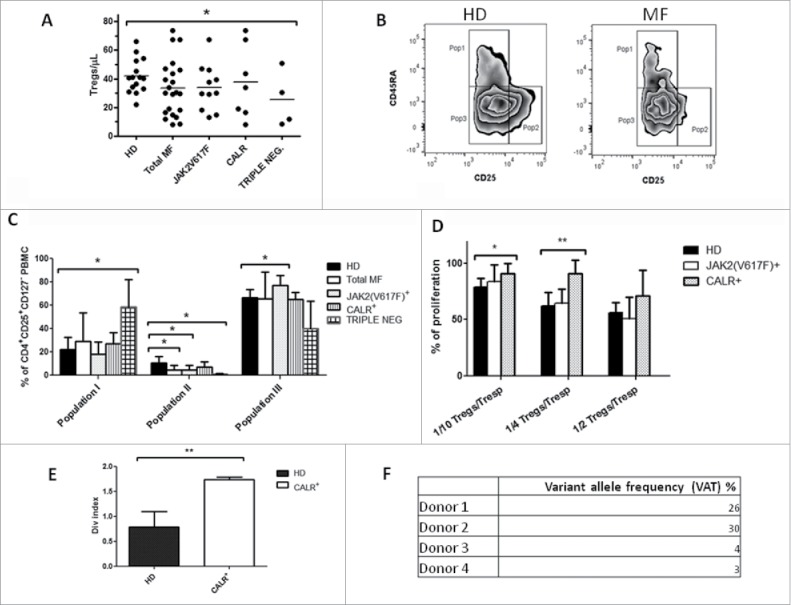
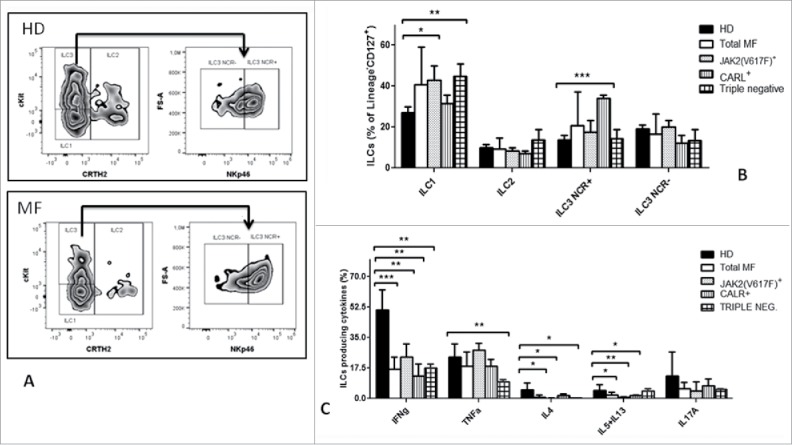
Myelofibrosis (MF) is a clonal neoplasia associated with chronic inflammation due to aberrant cytokine production. Mutations in Janus Kinase-2 (JAK2), calreticulin (CALR) and myeloproliferative leukemia protein (MPL) genes have been recently associated to MF and they all activate the JAK/STAT signaling pathway. Since this pathway is essential in shaping the immune response, we investigated the role of circulating immune subsets and cytokines in 38 patients (20 carrying JAK2(V617F),13 exon-9 CALR mutation and 5 triple negative). In comparison to healthy donors, patients presented a reduced amount of circulating dendritic cells (DCs) associated with a defective ability of monocytes in differentiating into DCs. In addition, we found a reduction in circulating T-helper (Th)1 and Th17 and hypo-functional innate lymphoid cells (ILC). Results analyzed according to the mutational status showed that patients carrying JAK2(V617F) mutation had a reduction in Th17, myeloid-DCs and effector Tregs as well as increased ILC1 and cytokine producing Tregs. The CALR mutated patients revealed high ILC3 levels, reduced Th1 and their monocytes had a reduced capacity to mature in vitro into fully committed DCs. Their Tregs were also less effective in inhibiting the proliferation of autologous effector T-cells due to an increased proliferative status induced by CALR mutation. Triple negative patients presented a reduced amount of total circulating CD3, effectors Tregs and Th1 with increased ILC1. Overall, we have demonstrated that in MF different mutations lead to phenotypic and functional alterations in different immune subsets that may have a potential role in disease progression and susceptibility to infections.
Keywords: Calreticulin; Immune dysregulation; JAK2(V617F); Myelofibrosis; chronic inflammation.
Figures
References
-
- Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz MJ, Porwit A, Harris NL, Le Beau MM, Hellström-Lindberg E, Tefferi A, et al.. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood 2009; 114:937-51; https://doi.org/ 10.1182/blood-2009-03-209262 - DOI - PubMed
-
- James C, Ugo V, Casadevall N, Constantinescu SN, Vainchenker W. A JAK2 mutation in myeloproliferative disorders: pathogenesis and therapeutic and scientific prospects. Trends Mol Med 2005; 11:546-54; https://doi.org/ 10.1016/j.molmed.2005.10.003 - DOI - PubMed
-
- Lavi N. Calreticulin mutations in myeloproliferative neoplasms. Rambam Maimonides Med J 2014; 5:e0035; PMID:25386351; https://doi.org/ 10.5041/RMMJ.10169 - DOI - PMC - PubMed
-
- Rampal R, Al-Shahrour F, Abdel-Wahab O, Patel JP, Brunel JP, Mermel CH, Bass AJ, Pretz J, Ahn J, Hricik T, et al.. Integrated genomic analysis illustrates the central role of JAK-STAT pathway activation in myeloproliferative neoplasm pathogenesis. Blood 2014; 123:e123-33; PMID:24740812; https://doi.org/ 10.1182/blood-2014-02-554634 - DOI - PMC - PubMed
-
- Passamonti F, Cervantes F, Vannucchi AM, Morra E, Rumi E, Pereira A, Guglielmelli P, Pungolino E, Caramella M, Maffioli M, et al.. A dynamic prognostic model to predict survival in primary myelofibrosis: a study by the IWG-MRT (International Working Group for Myeloproliferative Neoplasms Research and Treatment). Blood 2010; 115:1703-8; PMID:20008785; https://doi.org/ 10.1182/blood-2009-09-245837 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous