Femoro-Supragenicular Popliteal Bypass with a Bridging Stent Graft in a Diffusely Diseased Distal Target Popliteal Artery: Alternative to Below-Knee Popliteal Polytetrafluoroethylene Bypass
- PMID: 29124029
- PMCID: PMC5628965
- DOI: 10.5090/kjtcs.2017.50.5.371
Femoro-Supragenicular Popliteal Bypass with a Bridging Stent Graft in a Diffusely Diseased Distal Target Popliteal Artery: Alternative to Below-Knee Popliteal Polytetrafluoroethylene Bypass
Abstract
Background: Lesions in distal target arteries hinder surgical bypass procedures in patients with peripheral arterial occlusive disease.
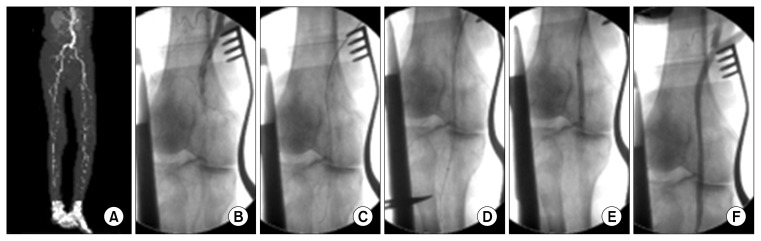
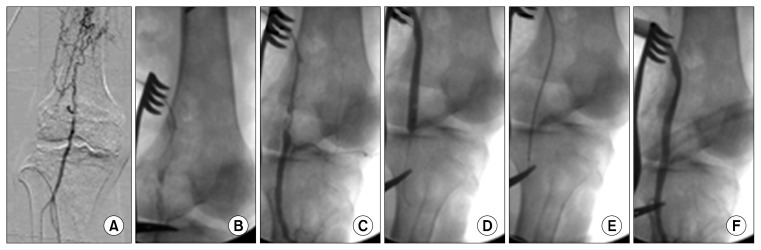
Methods: Between April 2012 and October 2015, 16 patients (18 limbs) with lifestyle-limiting claudication (n=12) or chronic critical limb ischemia (n=6) underwent femoral-above-knee (AK) polytetrafluoroethylene (PTFE) bypass grafts with a bridging stent graft placement between the distal target popliteal artery and the PTFE graft. Ring-supported PTFE grafts were used in all patients with no available vein for graft material. Follow-up evaluations assessed clinical symptoms, the ankle-brachial index, ultrasonographic imaging and/or computed tomography angiography, the primary patency rate, and complications.
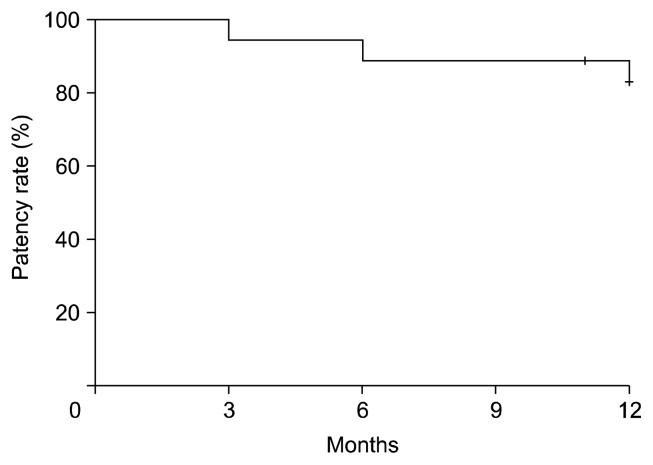
Results: All procedures were successful. The mean follow-up was 12.6 months (range, 11 to 14 months), and there were no major complications. The median baseline ankle-brachial index of 0.4 (range, 0.2 to 0.55) significantly increased to 0.8 (range, 0.5 to 1.0) at 12 months (p<0.01). The primary patency rate at 12 months was 83.3%. The presenting symptoms resolved within 2 weeks.
Conclusion: In AK bypasses with a diffusely diseased distal target popliteal artery or when below-knee (BK) bypass surgery is impossible, this procedure could be clinically effective and safe when used as an alternative to femoral-BK bypass surgery.
Keywords: Arteries; Bypass; Graft; Stents.
Conflict of interest statement
Conflict of interest No potential conflicts of interest relevant to this article are reported.
Figures
Similar articles
-
Randomized comparison of ePTFE/nitinol self-expanding stent graft vs prosthetic femoral-popliteal bypass in the treatment of superficial femoral artery occlusive disease.J Vasc Surg. 2009 Jan;49(1):109-15, 116.e1-9; discussion 116. doi: 10.1016/j.jvs.2008.08.041. Epub 2008 Nov 22. J Vasc Surg. 2009. PMID: 19028055 Clinical Trial.
-
[Factors determining late patency of aortobifemoral bypass graft].Srp Arh Celok Lek. 1997 Jan-Feb;125(1-2):24-35. Srp Arh Celok Lek. 1997. PMID: 17974352 Serbian.
-
Four-year randomized prospective comparison of percutaneous ePTFE/nitinol self-expanding stent graft versus prosthetic femoral-popliteal bypass in the treatment of superficial femoral artery occlusive disease.J Vasc Surg. 2010 Sep;52(3):584-90; discussion 590-1, 591.e1-591.e7. doi: 10.1016/j.jvs.2010.03.071. J Vasc Surg. 2010. PMID: 20598480 Clinical Trial.
-
A meta-analysis to compare Dacron versus polytetrafluroethylene grafts for above-knee femoropopliteal artery bypass.J Vasc Surg. 2014 Aug;60(2):506-15. doi: 10.1016/j.jvs.2014.05.049. Epub 2014 Jun 25. J Vasc Surg. 2014. PMID: 24973288 Review.
-
Popliteal artery aneurysms. Factors associated with thromboembolism and graft failure.Int Angiol. 2004 Mar;23(1):54-65. Int Angiol. 2004. PMID: 15156131 Review.
References
-
- Kim HY, Kim JS, Kim MY, Hwang SW, Yoo BH. Comparison of saphenous vein and PTFE grafts for above the knee femoropopliteal bypass grafting. Korean J Thorac Cardiovasc Surg. 2010;43:127–32. doi: 10.5090/kjtcs.2010.43.2.127. - DOI
-
- Baumann F, Do DD, Willenberg T, Baumgartner I, Diehm N. Treatment for long-segment femoro-popliteal obstructions: initial experience with a 4-F compatible self-expanding nitinol stent and review of the literature. J Cardiovasc Surg (Torino) 2012;53:475–80. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous