

Labor Induction with Orally Administrated Misoprostol: A Retrospective Cohort Study
- PMID: 29124067
- PMCID: PMC5624161
- DOI: 10.1155/2017/6840592
Labor Induction with Orally Administrated Misoprostol: A Retrospective Cohort Study
Abstract
Introduction: One great challenge in obstetric care is labor inductions. Misoprostol has advantages in being cheap and stable at room temperature and available in resource-poor settings.
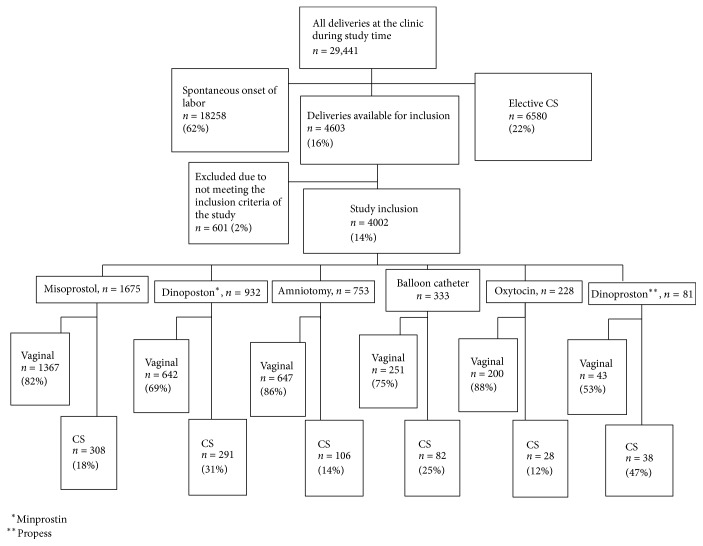
Material and methods: Retrospective cohort study of 4002 singleton pregnancies with a gestational age ≥34 w at Sodersjukhuset, Stockholm, during 2009-2010 and 2012-2013. Previously used methods of labor induction were compared with misoprostol given as a solution to drink, every second hour. Main outcome is as follows: Cesarean Section (CS) rate, acid-base status in cord blood, Apgar score < 7,5', active time of labor, and blood loss > 1500 ml (PPH).
Results: The proportion of CS decreased from 26% to 17% when orally given solution of misoprostol was introduced at the clinic (p < 0.001). No significant difference in the frequency of low Apgar score (p = 0.3), low aPh in cord blood (p = 0.1), or PPH (p = 0.4) between the different methods of induction was studied. After adjustment for different risk factor for CS the only method of induction which was associated with CS was dinoproston⁎⁎ (Propess®) (aor = 2.9 (1.6-5.2)).
Conclusion: Induction of labor with misoprostol, given as an oral solution to drink every second hour, gives a low rate of CS, without affecting maternal or fetal outcome.
Similar articles
-
Safety of misoprostol for near-term and term induction in small-for-gestational-age pregnancies compared to dinoprostone and primary cesarean section: results of a retrospective cohort study.Arch Gynecol Obstet. 2020 Dec;302(6):1369-1374. doi: 10.1007/s00404-020-05703-2. Epub 2020 Aug 5. Arch Gynecol Obstet. 2020. PMID: 32761274
-
An audit of oral administration of Angusta® (misoprostol) 25 µg for induction of labor in 976 consecutive women with a singleton pregnancy in a university hospital in Denmark.Acta Obstet Gynecol Scand. 2020 Oct;99(10):1396-1402. doi: 10.1111/aogs.13876. Epub 2020 May 19. Acta Obstet Gynecol Scand. 2020. PMID: 32311758
-
Induction of labor with high- or low-dosage oral misoprostol-A Danish descriptive retrospective cohort study 2015-16.Acta Obstet Gynecol Scand. 2020 Feb;99(2):222-230. doi: 10.1111/aogs.13739. Epub 2019 Oct 21. Acta Obstet Gynecol Scand. 2020. PMID: 31557305
-
Slow-release vaginal insert of misoprostol versus orally administrated solution of misoprostol for the induction of labour in primiparous term pregnant women: a randomised controlled trial.BJOG. 2019 Aug;126(9):1148-1155. doi: 10.1111/1471-0528.15796. Epub 2019 May 15. BJOG. 2019. PMID: 30989788 Clinical Trial.
-
[Use of misoprostol for induction of labor in case of fetal death or termination of pregnancy during second or third trimester of pregnancy: Efficiency, dosage, route of administration, side effects, use in case of uterine scar].J Gynecol Obstet Biol Reprod (Paris). 2014 Feb;43(2):146-61. doi: 10.1016/j.jgyn.2013.11.008. Epub 2014 Jan 22. J Gynecol Obstet Biol Reprod (Paris). 2014. PMID: 24461423 Review. French.
Cited by
-
Sublingual misoprostol vs. oral misoprostol solution for induction of labor: A retrospective study.Front Surg. 2022 Sep 15;9:968372. doi: 10.3389/fsurg.2022.968372. eCollection 2022. Front Surg. 2022. PMID: 36189381 Free PMC article.
-
A comparative analysis of methods of preinduction cervical ripening and induction of labor in Poland and in Germany (Part II): maternal and neonatal outcomes.BMC Pregnancy Childbirth. 2025 Jan 27;25(1):72. doi: 10.1186/s12884-024-07015-8. BMC Pregnancy Childbirth. 2025. PMID: 39871179 Free PMC article.
-
Factors of Non-Compliance with a Protocol for Oral Administration of Misoprostol (Angusta®) 25 Micrograms to Induce Labor: An Observational Study.J Clin Med. 2023 Feb 14;12(4):1521. doi: 10.3390/jcm12041521. J Clin Med. 2023. PMID: 36836056 Free PMC article.
-
Comparison of the Efficacy and Safety of Sublingual Versus Oral Misoprostol for the Induction of Labor: A Randomized Open-Label Study.Cureus. 2023 Nov 26;15(11):e49422. doi: 10.7759/cureus.49422. eCollection 2023 Nov. Cureus. 2023. PMID: 38149157 Free PMC article.
References
-
- Alkema L., Chou D., Hogan D., et al. Global, regional, and national levels and trends in maternal mortality between 1990 and 2015, with scenario-based projections to 2030: a systematic analysis by the un Maternal Mortality Estimation Inter-Agency Group. The Lancet. 2016;387(10017):462–474. doi: 10.1016/S0140-6736(15)00838-7. - DOI - PMC - PubMed
-
- WHO. Guidelines Approved by the Guidelines Review Committee. Geneva, Switzerland: World Health Organization; 2011.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
