

Understanding the aetiology and resolution of chronic otitis media from animal and human studies
- PMID: 29125825
- PMCID: PMC5719252
- DOI: 10.1242/dmm.029983
Understanding the aetiology and resolution of chronic otitis media from animal and human studies
Abstract
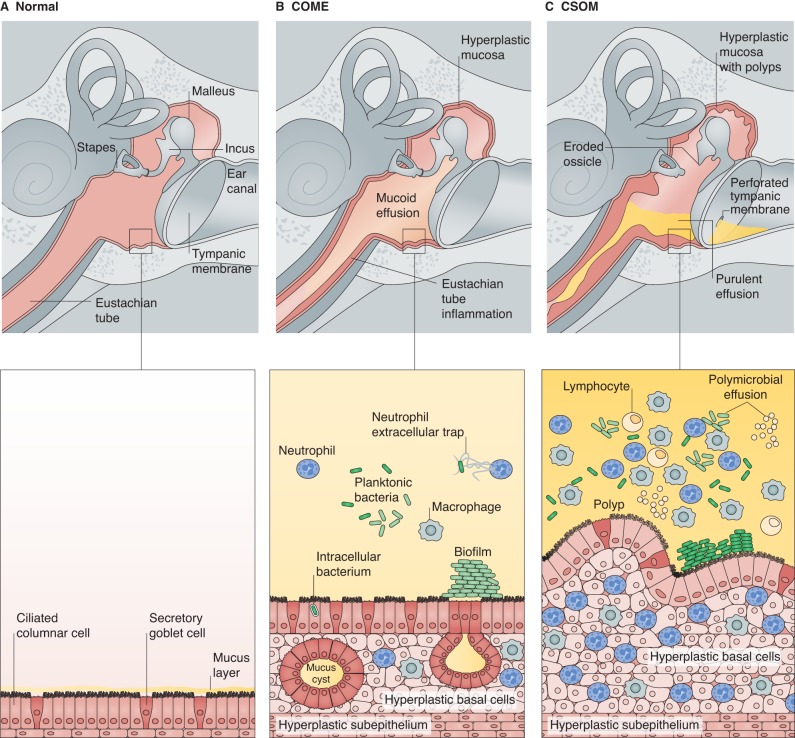
Inflammation of the middle ear, known clinically as chronic otitis media, presents in different forms, such as chronic otitis media with effusion (COME; glue ear) and chronic suppurative otitis media (CSOM). These are highly prevalent diseases, especially in childhood, and lead to significant morbidity worldwide. However, much remains unclear about this disease, including its aetiology, initiation and perpetuation, and the relative roles of mucosal and leukocyte biology, pathogens, and Eustachian tube function. Chronic otitis media is commonly modelled in mice but most existing models only partially mimic human disease and many are syndromic. Nevertheless, these models have provided insights into potential disease mechanisms, and have implicated altered immune signalling, mucociliary function and Eustachian tube function as potential predisposing mechanisms. Clinical studies of chronic otitis media have yet to implicate a particular molecular pathway or mechanism, and current human genetic studies are underpowered. We also do not fully understand how existing interventions, such as tympanic membrane repair, work, nor how chronic otitis media spontaneously resolves. This Clinical Puzzle article describes our current knowledge of chronic otitis media and the existing research models for this condition. It also identifies unanswered questions about its pathogenesis and treatment, with the goal of advancing our understanding of this disease to aid the development of novel therapeutic interventions.
Keywords: Animal models; Chronic otitis media; Genetics; Inflammation.
© 2017. Published by The Company of Biologists Ltd.
Conflict of interest statement
Competing interestsThe authors declare no competing or financial interests.
Figures
Similar articles
-
The significance of experimental animal studies in otitis media.Otolaryngol Clin North Am. 1991 Aug;24(4):813-27. Otolaryngol Clin North Am. 1991. PMID: 1870875 Review.
-
Otitis media: pathogenesis and medical sequelae.Ear Nose Throat J. 1998 Jun;77(6 Suppl):3-6. Ear Nose Throat J. 1998. PMID: 9674327 Review.
-
Mouse models of otitis media.Curr Opin Otolaryngol Head Neck Surg. 2006 Oct;14(5):341-6. doi: 10.1097/01.moo.0000244193.97301.d7. Curr Opin Otolaryngol Head Neck Surg. 2006. PMID: 16974149 Review.
-
[Physiopathology of inflammation of the middle ear].Rev Prat. 1998 Apr 15;48(8):833-7. Rev Prat. 1998. PMID: 11767325 French.
-
C3H/HeJ mouse model for spontaneous chronic otitis media.Laryngoscope. 2006 Jul;116(7):1071-9. doi: 10.1097/01.mlg.0000224527.41288.c4. Laryngoscope. 2006. PMID: 16826039
Cited by
-
Serous otitis media: Clinical and therapeutic considerations, including dexamethasone (C22H29FO5) intratympanic injection.Exp Ther Med. 2022 Feb;23(2):125. doi: 10.3892/etm.2021.11048. Epub 2021 Dec 7. Exp Ther Med. 2022. PMID: 34970348 Free PMC article.
-
Current Understanding of Host Genetics of Otitis Media.Front Genet. 2020 Feb 7;10:1395. doi: 10.3389/fgene.2019.01395. eCollection 2019. Front Genet. 2020. PMID: 32117425 Free PMC article. Review.
-
[Current hypotheses on the development of chronic otitis media with effusion in childhood].HNO. 2025 Apr;73(4):271-282. doi: 10.1007/s00106-025-01571-x. Epub 2025 Feb 28. HNO. 2025. PMID: 40019513 Review. German.
-
Establishment of novel immortalized middle ear cell lines as models for otitis media.Laryngoscope Investig Otolaryngol. 2023 Aug 28;8(5):1428-1435. doi: 10.1002/lio2.1141. eCollection 2023 Oct. Laryngoscope Investig Otolaryngol. 2023. PMID: 37899851 Free PMC article.
-
Chronic otitis media is initiated by a bulla cavitation defect in the FBXO11 mouse model.Dis Model Mech. 2019 Mar 21;12(3):dmm038315. doi: 10.1242/dmm.038315. Dis Model Mech. 2019. PMID: 30898767 Free PMC article.
References
-
- Allen E. K., Chen W.-M., Weeks D. E., Chen F., Hou X., Mattos J. L., Mychaleckyj J. C., Segade F., Casselbrant M. L., Mandel E. M. et al. (2013). A genome-wide association study of chronic otitis media with effusion and recurrent otitis media identifies a novel susceptibility locus on chromosome 2. J. Assoc. Res. Otolaryngol. 14, 791-800. 10.1007/s10162-013-0411-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
