

Analysis of a Screening System for Diabetic Cardiovascular Autonomic Neuropathy in China
- PMID: 29125834
- PMCID: PMC5694192
- DOI: 10.12659/msm.905240
Analysis of a Screening System for Diabetic Cardiovascular Autonomic Neuropathy in China
Abstract
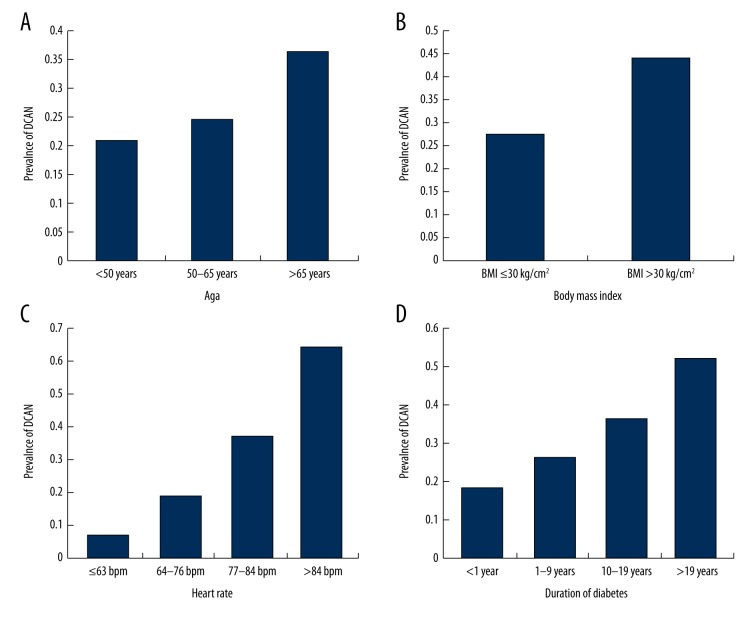
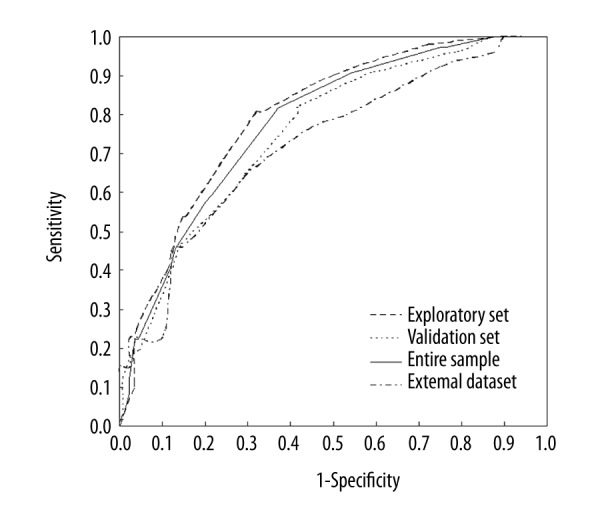
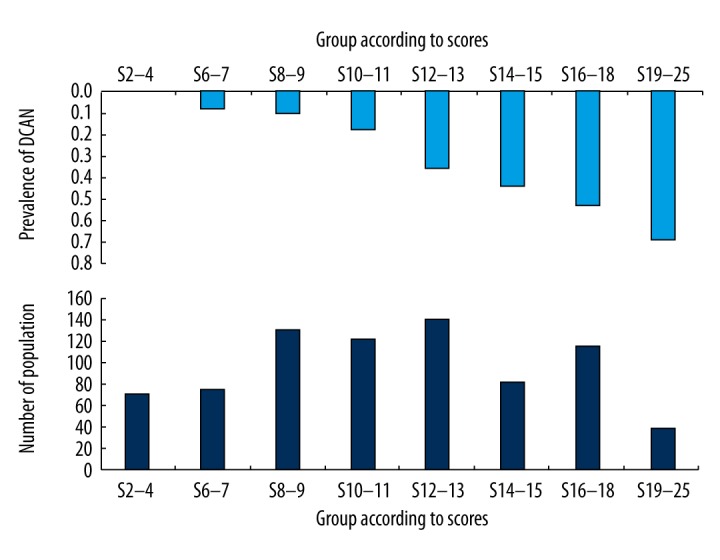
BACKGROUND The aim of this study was to create a screening system for diabetic cardiovascular autonomic neuropathy (DCAN) in diabetic patients. MATERIAL AND METHODS A Chinese cohort of 455 diabetic participants was recruited between 2011 and 2013. Short-term heart rate variability testing was used to evaluate cardiovascular autonomic function. A simple model was developed using multiple variable regression to include only significant risk factors that were simple and easily assessed. A DCAN score was determined based on the coefficients of the multiple variable model. This score was tested on the entire cohort of 455 diabetic patients and another independent, external cohort of 115 diabetic patients. RESULTS The screening system consisted of age, body mass index, duration of diabetes mellitus, and resting heart rate, and these factors were significantly (P<0.05) associated with DCAN. Receiver operating characteristic (ROC) curve analysis was done. The areas under the ROC curve were 0.798, 0.756, and 0.729 for the total sample, validation cohort, and external set, respectively. A cutoff DCAN score of 12 out of 25 produced optimal results for sensitivity (80.36%), specificity (58.27%), and percentage of patients that needed subsequent testing (43.55%) for the validation set. CONCLUSIONS The study concludes that a simple and practical DCAN screening can be applied for early intervention to delay or prevent the disease in the Chinese population.
Conflict of interest statement
None.
Figures
References
-
- Vinik AI, Maser RE, Mitchell BD, Freeman R. Diabetic autonomic neuropathy. Diabetes Care. 2003;26:1553–79. - PubMed
-
- Maser RE, Mitchell BD, Vinik AI, Freeman R. The association between cardiovascular autonomic neuropathy and mortality in individuals with diabetes: A meta-analysis. Diabetes Care. 2003;26:1895–901. - PubMed
-
- Hazari MA, Khan RT, Reddy BR, Hassan MA. Cardiovascular autonomic dysfunction in type 2 diabetes mellitus and essential hypertension in a South Indian population. Neurosciences. 2012;17:173–75. - PubMed
-
- Spallone V, Ziegler D, Freeman R, et al. Toronto Consensus Panel on Diabetic Neuropathy. Cardiovascular autonomic neuropathy in diabetes: Clinical impact, assessment, diagnosis, and management. Diabetes Metab Res Rev. 2011;27:639–53. - PubMed
-
- Banthia S, Bergner DW, Chicos AB, et al. Detection of cardiovascular autonomic neuropathy using exercise testing in patients with type 2 diabetes mellitus. J Diabetes Complications. 2013;27:64–69. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
