

A randomized phase II study of everolimus in combination with chemoradiation in newly diagnosed glioblastoma: results of NRG Oncology RTOG 0913
- PMID: 29126203
- PMCID: PMC5892159
- DOI: 10.1093/neuonc/nox209
A randomized phase II study of everolimus in combination with chemoradiation in newly diagnosed glioblastoma: results of NRG Oncology RTOG 0913
Abstract
Background: This phase II study was designed to determine the efficacy of the mammalian target of rapamycin (mTOR) inhibitor everolimus administered daily with conventional radiation therapy and chemotherapy in patients with newly diagnosed glioblastoma.
Methods: Patients were randomized to radiation therapy with concurrent and adjuvant temozolomide with or without daily everolimus (10 mg). The primary endpoint was progression-free survival (PFS) and the secondary endpoints were overall survival (OS) and treatment-related toxicities.
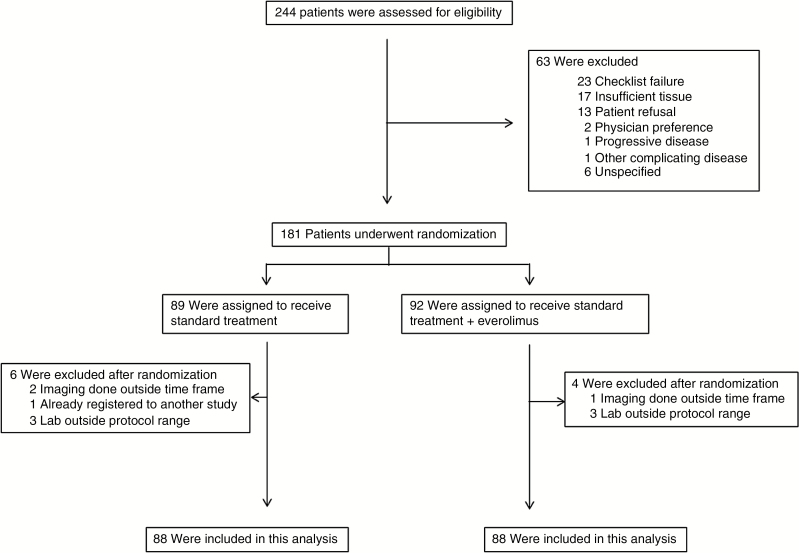
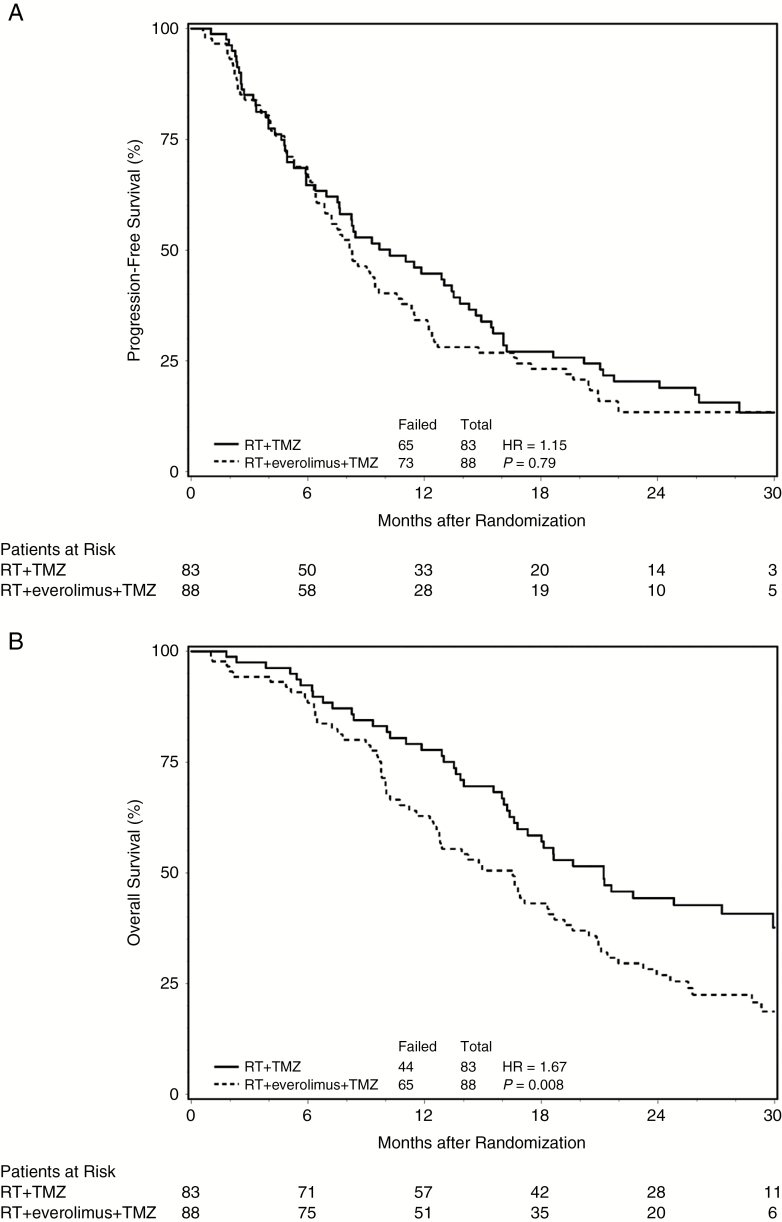
Results: A total of 171 patients were randomized and deemed eligible for this study. Patients randomized to receive everolimus experienced a significant increase in both grade 4 toxicities, including lymphopenia and thrombocytopenia, and treatment-related deaths. There was no significant difference in PFS between patients randomized to everolimus compared with control (median PFS time: 8.2 vs 10.2 mo, respectively; P = 0.79). OS for patients randomized to receive everolimus was inferior to that for control patients (median survival time: 16.5 vs 21.2 mo, respectively; P = 0.008). A similar trend was observed in both O6-methylguanine-DNA-methyltransferase promoter hypermethylated and unmethylated tumors.
Conclusion: Combining everolimus with conventional chemoradiation leads to increased treatment-related toxicities and does not improve PFS in patients with newly diagnosed glioblastoma. Although the median survival time in patients receiving everolimus was comparable to contemporary studies, it was inferior to the control in this randomized study.
Figures
Comment in
-
mTOR inhibition in glioblastoma: requiem for a dream?Neuro Oncol. 2018 Apr 9;20(5):584-585. doi: 10.1093/neuonc/noy034. Neuro Oncol. 2018. PMID: 29608764 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
