

Optimizing Tuberculosis Diagnosis in Human Immunodeficiency Virus-Infected Inpatients Meeting the Criteria of Seriously Ill in the World Health Organization Algorithm
- PMID: 29126226
- PMCID: PMC5905585
- DOI: 10.1093/cid/cix988
Optimizing Tuberculosis Diagnosis in Human Immunodeficiency Virus-Infected Inpatients Meeting the Criteria of Seriously Ill in the World Health Organization Algorithm
Abstract
Background: The World Health Organization (WHO) algorithm for the diagnosis of tuberculosis in seriously ill human immunodeficiency virus (HIV)-infected patients lacks a firm evidence base. We aimed to develop a clinical prediction rule for the diagnosis of tuberculosis and to determine the diagnostic utility of the Xpert MTB/RIF assay in seriously ill HIV-infected patients.
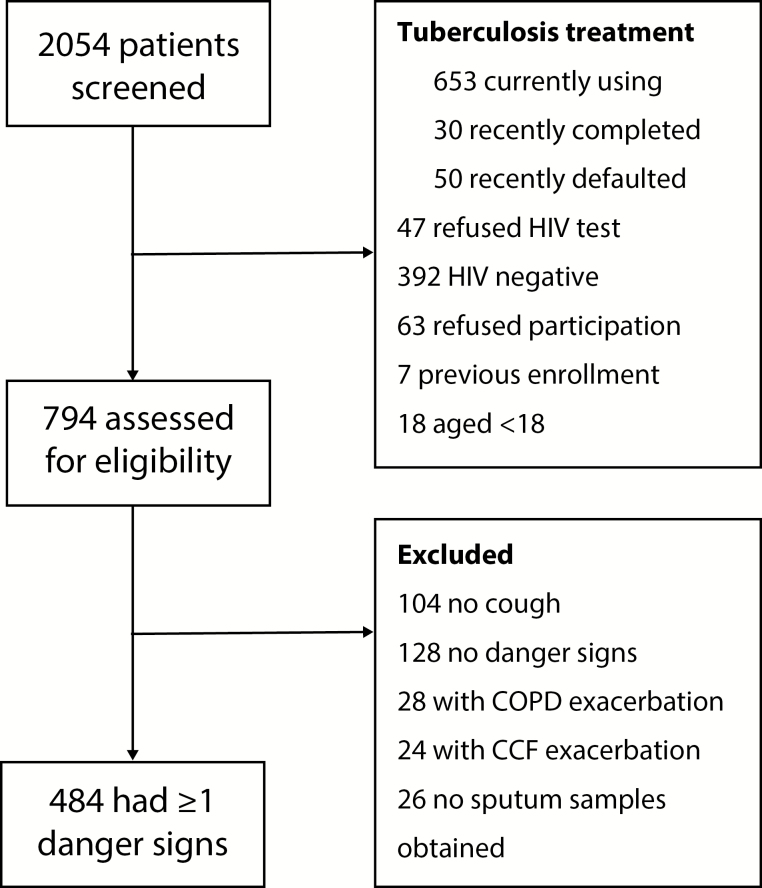
Methods: We conducted a prospective study among HIV-infected inpatients with any cough duration and WHO-defined danger signs. Culture-positive tuberculosis from any site was the reference standard. A priori selected variables were assessed for univariate associations with tuberculosis. The most predictive variables were assessed in a multivariate logistic regression model and used to establish a clinical prediction rule for diagnosing tuberculosis.
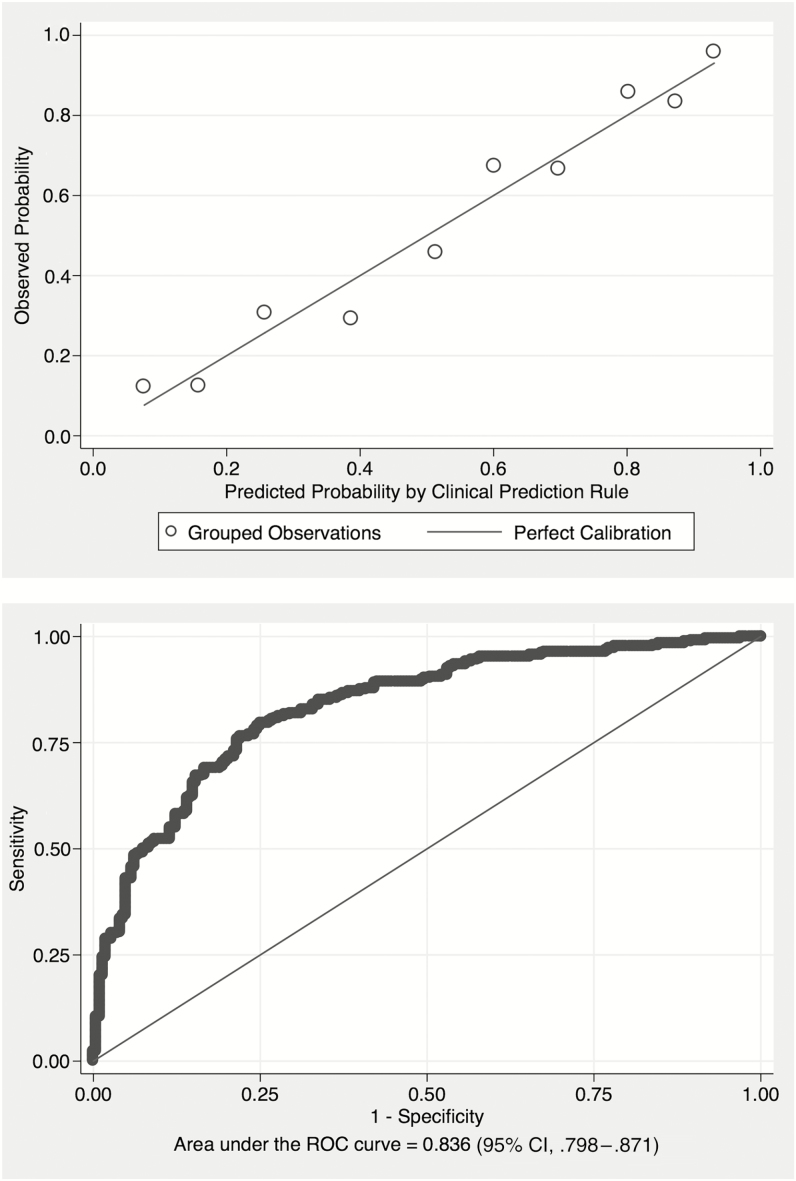
Results: We enrolled 484 participants. The median age was 36 years, 65.5% were female, the median CD4 count was 89 cells/µL, and 35.3% were on antiretroviral therapy. Tuberculosis was diagnosed in 52.7% of participants. The c-statistic of our clinical prediction rule (variables: cough ≥14 days, unable to walk unaided, temperature >39°C, chest radiograph assessment, hemoglobin, and white cell count) was 0.811 (95% confidence interval, .802-.819). The classic tuberculosis symptoms (fever, night sweats, weight loss) added no discriminatory value in diagnosing tuberculosis. Xpert MTB/RIF assay sensitivity was 86.3% and specificity was 96.1%.
Conclusions: Our clinical prediction rule had good diagnostic utility for tuberculosis among seriously ill HIV-infected inpatients. Xpert MTB/RIF assay, incorporated into the updated 2016 WHO algorithm, had high sensitivity and specificity in this population. Our findings could facilitate improved diagnosis of tuberculosis among seriously ill HIV-infected inpatients in resource-constrained settings.
Figures
References
-
- Getahun H, Harrington M, O’Brien R, Nunn P. Diagnosis of smear-negative pulmonary tuberculosis in people with HIV infection or AIDS in resource-constrained settings: informing urgent policy changes. Lancet 2007; 369:2042–9. - PubMed
-
- World Health Organization (WHO). Improving the diagnosis and treatment of smear-negative pulmonary and extra pulmonary tuberculosis among adults and adolescents, recommendations for HIV-prevalent and resource-constrained settings. WHO/HTM/TB/2007.379 Geneva, Switzerland: WHO, 2007.
-
- Holtz TH, Kabera G, Mthiyane T et al. . Use of a WHO-recommended algorithm to reduce mortality in seriously ill patients with HIV infection and smear-negative pulmonary tuberculosis in South Africa: an observational cohort study. Lancet Infect Dis 2011; 11:533–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
