

Concomitant glenohumeral pathologies in high-grade acromioclavicular separation (type III - V)
- PMID: 29126408
- PMCID: PMC5681781
- DOI: 10.1186/s12891-017-1803-y
Concomitant glenohumeral pathologies in high-grade acromioclavicular separation (type III - V)
Abstract
Background: Acromioclavicular joint (ACJ) dislocations are common injuries of the shoulder associated with physical activity. The diagnosis of concomitant injuries proves complicated due to the prominent clinical symptoms of acute ACJ dislocation. Because of increasing use of minimally invasive surgery techniques concomitant pathologies are diagnosed more often than with previous procedures.
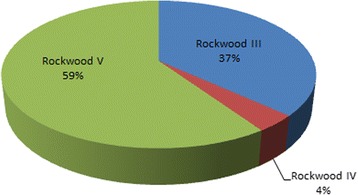
Methods: The aim of this study was to identify the incidence of concomitant intraarticular injuries in patients with high-grade acromioclavicular separation (Rockwood type III - V) as well as to reveal potential risk constellations. The concomitant pathologies were compiled during routine arthroscopically assisted treatment in altogether 163 patients (147 male; 16 female; mean age 36.8 years) with high-grade acromioclavicular separation (Rockwood type III: n = 60; Rockwood type IV: n = 6; Rockwood type V: n = 97).
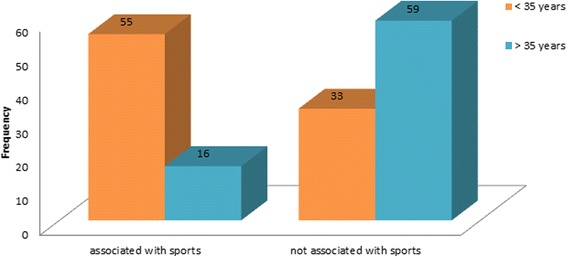
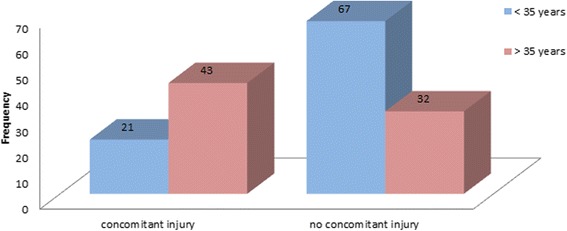
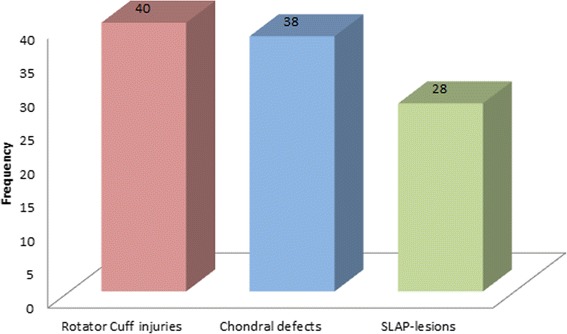
Results: Acromioclavicular separation occurred less often in women than men (1:9). In patients under 35, the most common cause for ACJ dislocation was sporting activity (37.4%). Rockwood type V was observed significantly more often than the other types with 57.5% (Rockwood type III = 36.8%, Rockwood type IV 3.7%). Concomitant pathologies were diagnosed in 39.3% of the patients with that number rising to as much as 57.3% in patients above 35 years. Most common associated injuries were rotator cuff injuries (32.3%), chondral defects (30.6%) and SLAP-lesions (22.6%). Of all patients, 8.6% needed additional reconstructive surgery.
Conclusion: Glenohumeral injuries are a much more common epiphenomenon during acromioclavicular separation than previously ascertained. High risk group for accompanying injuries are patients above 35 years with preexisting degenerative disease. The increasing use of minimally invasive techniques allows for an easier diagnosis and simultaneous treatment of the additional pathologies.
Keywords: Acromio-clavicular joint separation; Concomitant injuries; Shoulder arthroscopy.
Conflict of interest statement
Ethics approval and consent to participate
The ethical committee of the faculty of medicine of the Philipps-University Marburg, Germany, reference no. ek_mr_22_6_2017, was informed and ruled that no formal ethical approval was required in this particular study. Concerning the informed consent was deemed unnecessary according the ethical committee in the same approval mentioned above due to retrospective design of the study with anonymised data and no patient involvement, as stated in the approval letter.
Consent for publication
not applicable.
Competing interests
The authors declare that they have no competing interests’ in relation to this study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Flatow EL. The biomechanics of the acromioclavicular, sternoclavicular, and scapulothoracic joints. Instructional course lectures 42, S. 1993:237–45. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
