

Obstetric fistulae in southern Mozambique: incidence, obstetric characteristics and treatment
- PMID: 29126412
- PMCID: PMC5681779
- DOI: 10.1186/s12978-017-0408-0
Obstetric fistulae in southern Mozambique: incidence, obstetric characteristics and treatment
Abstract
Background: Obstetric fistula is one of the most devastating consequences of unmet needs in obstetric services. Systematic reviews suggest that the pooled incidence of fistulae in community-based studies is 0.09 per 1000 recently pregnant women; however, as facility delivery is increasing, for the most part, in Africa, incidence of fistula should decrease. Few population-based studies on fistulae have been undertaken in Sub-Saharan Africa, including Mozambique. This study aimed to estimate the incidence of obstetric fistulae in recently delivered mothers, and to describe the clinical characteristics and care, as well as the outcome, after surgical repair.
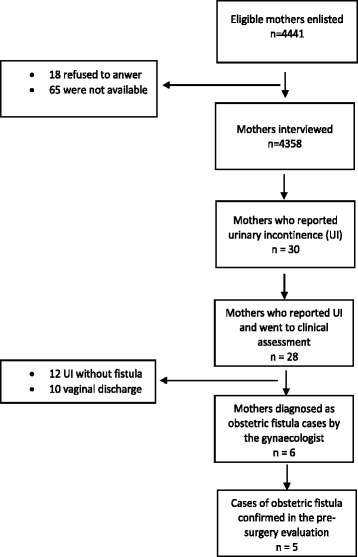
Methods: We selected women who had delivered up to 12 months before the start of the study (June, 1st 2016). They were part of a cohort of women of reproductive age (12-49 years), recruited from selected clusters in rural areas of Maputo and Gaza provinces, Southern Mozambique, who were participating in an intervention trial (the Community Level Interventions for Pre-eclampsia trial or CLIP trial). Case identification was completed by self-reported constant urine leakage and was confirmed by clinical assessment. Women who had confirmed obstetric fistulae were referred for surgical repair. Data were entered into a REDCap database and analysed using R software.
Results: Five women with obstetric fistulae were detected among 4358 interviewed, giving an incidence of 1.1 per 1000 recently pregnant women (95% CI 2.16-0.14). All but one had Caesarean section and all of the babies died. Four were stillborn, and one died very soon after birth. All of the patients identified and reached the primary health facility in reasonable time. Delays occurred in the care: in diagnosis of obstructed labour, and in the decision to refer to the secondary or third-level hospital. All but one of the women were referred to surgical repair and the fistulae successfully closed.
Conclusion: This population-based study reports a high incidence of obstetric fistulae in an area with high numbers of facility births. Few first and second delays in reaching care, but many third delays in receiving care, were identified. This raises concerns for quality of care.
Keywords: Caesarean; Incidence; Obstetric fistula; Population-based; Sub-Saharan Africa.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was provided by the Bioethics Review Joint Committee of the UEM Faculty of Medicine and Maputo Central Hospital (CIBS FM&HCM/33/2015, dated 28 August 2015). Informed consent was obtained from each participant before interview. Those aged less than 18 years were asked about their willingness to participate. Thereafter, informed consent was obtained from their parents or legal guardians, and additional assent was then obtained from those participants. For illiterate participants, a literate witness was involved in the consent process, the participant’s fingerprint was taken, and the consent form signed by the witness and the data collector. Women affected by obstetric fistula who presented themselves because of their awareness of the study but who did not fulfil the study inclusion criteria, were offered treatment.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Obstetric fistula in southern Mozambique: a qualitative study on women's experiences of care pregnancy, delivery and post-partum.Reprod Health. 2020 Jan 31;17(1):21. doi: 10.1186/s12978-020-0860-0. Reprod Health. 2020. PMID: 32005268 Free PMC article.
-
Obstetric fistula repair failure and its associated factors among women who underwent repair in sub-Saharan Africa. A systematic review and meta-analysis.PLoS One. 2024 Feb 5;19(2):e0295000. doi: 10.1371/journal.pone.0295000. eCollection 2024. PLoS One. 2024. PMID: 38315695 Free PMC article.
-
Obstetric fistula in 14,928 Ethiopian women.Acta Obstet Gynecol Scand. 2010 Jul;89(7):945-51. doi: 10.3109/00016341003801698. Acta Obstet Gynecol Scand. 2010. PMID: 20397760
-
Obstetric fistulae: a study of women managed at the Monze Mission Hospital, Zambia.BJOG. 2007 Aug;114(8):1010-7. doi: 10.1111/j.1471-0528.2007.01353.x. Epub 2007 May 16. BJOG. 2007. PMID: 17506793
-
Genital fistulae. A continuing tragedy.J Obstet Gynaecol Res. 1999 Feb;25(1):1-7. doi: 10.1111/j.1447-0756.1999.tb01114.x. J Obstet Gynaecol Res. 1999. PMID: 10067006 Review. No abstract available.
Cited by
-
Estimating the cost for obstetric fistula repair in hospitals of Mozambique: a low-income country.Health Econ Rev. 2024 Aug 26;14(1):65. doi: 10.1186/s13561-024-00542-2. Health Econ Rev. 2024. PMID: 39186146 Free PMC article.
-
Obstetric fistula in southern Mozambique: a qualitative study on women's experiences of care pregnancy, delivery and post-partum.Reprod Health. 2020 Jan 31;17(1):21. doi: 10.1186/s12978-020-0860-0. Reprod Health. 2020. PMID: 32005268 Free PMC article.
-
Rectovaginal fistula in a patient with Mayer-Rokitansky-Kuster-Hauser syndrome.Urol Case Rep. 2025 May 21;61:103075. doi: 10.1016/j.eucr.2025.103075. eCollection 2025 Jul. Urol Case Rep. 2025. PMID: 40502923 Free PMC article.
-
Mothers' satisfaction with care during facility-based childbirth: a cross-sectional survey in southern Mozambique.BMC Pregnancy Childbirth. 2019 Aug 19;19(1):303. doi: 10.1186/s12884-019-2449-6. BMC Pregnancy Childbirth. 2019. PMID: 31426758 Free PMC article.
-
LUSSY score predictive of failure of surgical closure of obstetric rectovaginal fistula in the Democratic Republic of the Congo.Reprod Health. 2025 Mar 12;22(1):37. doi: 10.1186/s12978-025-01971-w. Reprod Health. 2025. PMID: 40069727 Free PMC article.
References
-
- WHO . Obstetric fistula: Guiding principles for clinical management and program development. Geneva: World Health Organization; 2006.
-
- De Ridder D, Badlani GH, Browning A, et al. Fistulas in the developing world. In: Abrams P, Cardozo L, Khoury S, Wein A, editors. Incontinence, 4th ed. Paris: Health Publications Ltd.; 2009. p. 1419–58.
-
- Neilson JP. Obstructed labor. Br Med Bull. 2003;67(1) - PubMed
-
- Wall LL, et al. The obstetric vesicovaginal fistula in the developing world. Obstet Gynecol Surv. 2005;60(7 Suppl 1):S3–S51. https://www.ncbi.nlm.nih.gov/m/pubmed/16034313/?i=4&from=/16895244/related. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
