

Failure to achieve lupus low disease activity state (LLDAS) six months after diagnosis is associated with early damage accrual in Caucasian patients with systemic lupus erythematosus
- PMID: 29126432
- PMCID: PMC5681839
- DOI: 10.1186/s13075-017-1451-5
Failure to achieve lupus low disease activity state (LLDAS) six months after diagnosis is associated with early damage accrual in Caucasian patients with systemic lupus erythematosus
Abstract
Background: The aim was to assess the attainability and outcome of the lupus low disease activity state (LLDAS) in the early stages of systemic lupus erythematosus (SLE).
Methods: LLDAS prevalence was evaluated at 6 (T1) and 18 (T2) months after diagnosis and treatment initiation (T0) in a monocentric cohort of 107 (median disease duration 9.7 months) prospectively followed Caucasian patients with SLE. Reasons for failure to achieve LLDAS were also investigated. Multivariate models were built to identify factors associated with lack of LLDAS achievement and to investigate the relationship between LLDAS and Systemic Lupus International Collaboration Clinics (SLICC)/Damage Index (SDI) accrual.
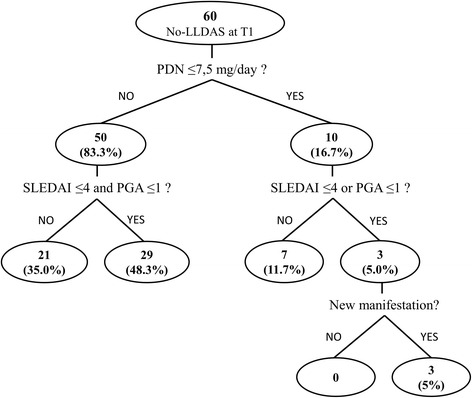
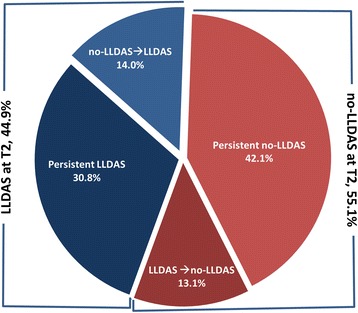
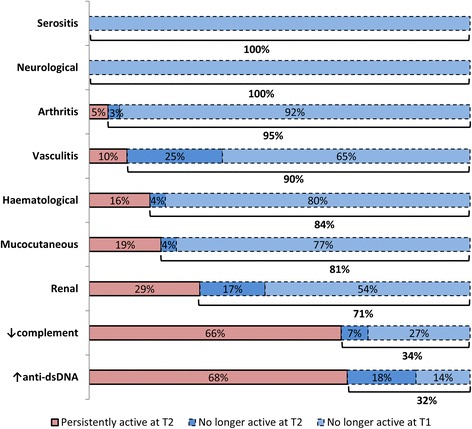
Results: There were 47 (43.9%) patients in LLDAS at T1 and 48 (44.9%) at T2. The most frequent unmet LLDAS criterion was prednisolone dose >7.5 mg/day (83% of patients with no LLDAS at T1). Disease manifestations with the lowest remission rate during follow up were increased anti-double-stranded DNA (persistently present in 85.7% and 67.5% of cases at T1 and T2, respectively), low serum complement fractions (73.2% and 66.3%) and renal abnormalities (46.4% and 28.6%). Renal involvement at T0 was significantly associated with failure to achieve LLDAS both at T1 (OR 7.8, 95% CI 1.4-43.4; p = 0.019) and T2 (OR 3.9, 95% CI 1.4-10.6; p = 0.008). Presence of any organ damage (SDI ≥1) at T2 was significantly associated with lack of LLDAS at T1 (OR 5.0, 95% CI 1.5-16.6; p = 0.009) and older age at diagnosis (OR 1.05 per year, 95% CI 1.01-1.09; p = 0.020).
Conclusion: LLDAS is a promising treatment target in the early stages of SLE, being attainable and negatively associated with damage accrual, but it fit poorly to patients with renal involvement.
Keywords: Disease activity; Outcomes research; Systemic lupus erythematosus.
Conflict of interest statement
Authors’ information
Not applicable.
Ethics approval and consent to participate
Ethical approval was obtained from local Azienda Ospedaliera Universitaria of Cagliari Ethics Committee and all participants gave their written informed consent.
Consent for publication
Consent for publication was obtained.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Doria A, Iaccarino L, La Montagna G, Mathieu A, Piga M, Galeazzi M, et al. Clinical profile and direct medical cost of care of adults presenting with systemic lupus erythematosus in Italy. Clin Exp Rheumatol. 2015;33:375–84. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
