

Detection level and pattern of positive lesions using PSMA PET/CT for staging prior to radiation therapy
- PMID: 29126446
- PMCID: PMC5681820
- DOI: 10.1186/s13014-017-0902-0
Detection level and pattern of positive lesions using PSMA PET/CT for staging prior to radiation therapy
Abstract
Background: To determine the potential role of 68Ga-PSMA positron emission tomography/computed tomography (PET/CT) in radiotherapy (RT) planning for prostate cancer (PCa).
Methods: One hundred twenty-nine patients (pts) with 68Ga-PSMA PET/CT were retrospectively analysed. Potentially influencing factors (androgen deprivation therapy, amount of 68Ga-PSMA-HBED-CC, PSA doubling time ≤/> 10 months, PSA before PET/CT, T-/N-category and Gleason score) were evaluated by logistic regression analysis. The detection rate of PSMA PET/CT was compared to contrast enhanced CT and its impact on RT management analysed.
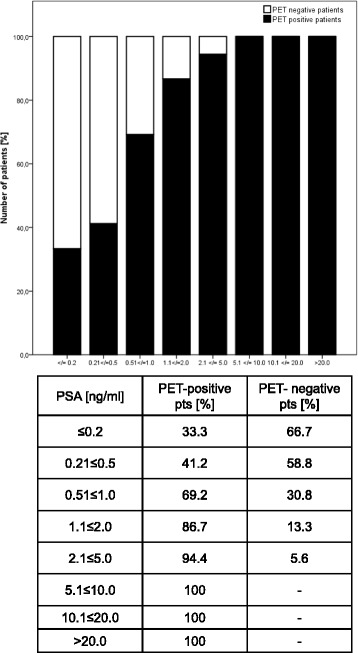
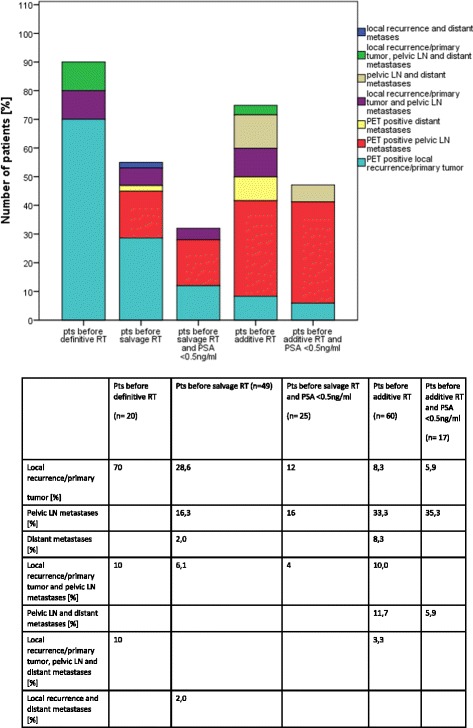
Results: One hundred twenty-nine patients (pts) (20 at initial diagnosis, 49 with PSA relapse and 60 with PSA persistence after radical prostatectomy) received PSMA PET/CT prior to RT. The majority of pts. (71.3%) had PET-positive findings (55.1% of pts. with PSA recurrence, 75% of pts. with PSA persistence and 100% of newly diagnosed pts). Median PSA before PET/CT in pts. with pathological findings (n = 92) was 1.90 ng/ml and without (n = 37) 0.30 ng/ml. PSA level at time of PET/CT was the only factor associated with PET-positivity. In pts. with a PSA ≤ 0.2 ng/ml, the detection rate of any lesion was 33.3%, with a PSA of 0.21-0.5 ng/ml 41.2% and with a PSA of 0.51-1.0 ng/ml 69.2%, respectively. Regarding the anatomic distribution of lesions, 42.2% and 14.7% of pts. with relapse or persistence had pelvic lymph node and distant metastases. In pts. at initial diagnosis the detection rate of pelvic lymph nodes and distant metastases was 20% and 10%. 68Ga-PSMA PET/CT had a high detection rate of PCa recurrence outside the prostatic fossa in pts. being considered for salvage RT (22.4% PET-positive pelvic lymph nodes and 4.1% distant metastases). Compared to CT, PSMA PET/CT had a significantly higher sensitivity in diagnosing rates of local recurrence/primary tumour (10.1% vs. 38%), lymph nodes (15.5% vs. 38.8%) and distant metastases (5.4% vs. 14.0%). This resulted in a modification of RT treatment in 56.6% of pts.
Conclusions: The detection of PCa is strongly associated with PSA level at time of 68Ga-PSMA PET/CT. PSMA PET/CT differentiates between local, regional and distant metastatic disease with implications for disease management. PSMA PET/CT allows for tumour detection in post-prostatectomy pts. with PSA ≤ 0.5 ng/ml considered for salvage RT.
Keywords: 68Ga-PSMA PET/CT; Prostate cancer; Radical prostatectomy; Radiotherapy.
Conflict of interest statement
Ethics approval and consent to participate
All patients gave written consent to undergo 68Ga-PSMA PET/CT. This retrospective analysis is in compliance with the principles of the Declaration of Helsinki and its subsequent amendments [21] and was approved by the Ethics Committee of the LMU Medical Faculty.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Schiller K, Sauter K, Dewes S, Eiber M, Maurer T, Gschwend J, Combs SE, et al. Patterns of failure after radical prostatectomy in prostate cancer - implications for radiation therapy planning after (68)Ga-PSMA-PET imaging. Eur J Nucl Med Mol Imaging. 2017; doi: 10.1007/s00259-017-3746-9. - PubMed
-
- Vargas HA, Martin-Malburet AG, Takeda T, Corradi RB, Eastham J, Wibmer A, et al. Localizing sites of disease in patients with rising serum prostate-specific antigen up to 1 ng/ml following prostatectomy: how much information can conventional imaging provide? Urol Oncol-Semin Orig Investig. 2016;34(11):482.e485-482.e410. - PMC - PubMed
-
- Panje C, Panje T, Putora PM, Kim SK, Haile S, Aebersold DM, et al. Guidance of treatment decisions in risk-adapted primary radiotherapy for prostate cancer using multiparametric magnetic resonance imaging: a single center experience. Radiat Oncol. 2015;10(1):47. doi: 10.1186/s13014-015-0338-3. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
